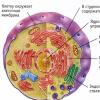
The height of the thoracic vertebrae is normal. The structure of the human vertebrae. The right working conditions
The spinal column consists of vertebrae assembled in an S-shaped structure, which ensures the musculoskeletal function of the entire skeleton.
The structure of the human vertebra is both simple and complex, so what parts it consists of and what function it performs will be discussed below.

The spine is the main part of the human skeleton, ideally adapted to perform a supporting function. Due to its unique structure and cushioning capabilities, the spine is able to distribute the load not only along its entire length, but also on other parts of the skeleton.
The spine consists of 32-33 vertebrae assembled into a mobile structure, inside which is the spinal cord, as well as nerve endings. Intervertebral discs are located between the vertebrae, thanks to which the spine has flexibility and mobility, and its bone parts do not touch each other.

Thanks to the structure of the spine ideally created by nature, it is able to ensure the normal functioning of a person. He is responsible for:
- creation of a reliable support during movement;
- proper functioning of organs;
- combining muscle and bone tissues into one system;
- protection of the spinal cord and vertebral artery.

The flexibility of the spine is developed individually for everyone, and depends primarily on the genetic predisposition, as well as on the type of human activity.

The spinal column is a skeleton for attaching muscle tissues, which in turn are a protective layer for it, as they take on external mechanical influences.
Support corset for the spine
Departments of the spine
The spine is divided into five sections.

Table number 1. The structure of the vertebrae. Characteristics and functions of departments.
| The Department | Number of vertebrae | Characteristic | Functions |
|---|---|---|---|
| 7 | The most mobile department. It has two vertebrae that are different from the rest. Atlas has no body, as it is formed by only two arcs. Has the shape of a ring. Epistropheus has a process that is associated with Atlas. | Atlas is responsible for supporting the head and tilting it forward. Axis (or epistropheus) helps with turning the head. | |
| 12 | It is considered the least mobile department. There are direct connections with ribs. This is achieved with the help of a special structure of the vertebrae themselves. The connection into one whole leads to the formation of a kind of protected space for the internal organs - the chest. | Organ protection, body support. | |
| 5 | It is called the working section of the spine. The lumbar vertebrae are distinguished by their massiveness and high strength. These two parameters are very important for the lower back, since all the main load falls on it. | Maintaining the body. | |
| 5 fused vertebrae | The sacrum is made up of five fused vertebrae, which in turn are fused with other bones to form the pelvis. | Maintaining the vertical position of the body and the distribution of loads. | |
| 4-5 | They are connected tightly and firmly. The main feature of the coccyx is its small process. It is called the coccygeal horn. The coccyx itself is a rudiment. | Protecting important parts of the body, attaching some muscles and ligaments. |
The structure of the vertebra
The vertebra is the main component of the spinal column.
In the center of each vertebrae there is a small opening called the spinal canal. It is reserved for the spinal cord and vertebral artery. They run through the entire spine. The connection of the spinal cord with the organs and limbs of the body is achieved through nerve endings.


Basically, the structure of the vertebrae is the same. Only fused areas and a couple of vertebrae, designed to perform certain functions, differ.
The vertebra consists of the following elements:
- body;
- legs (on both sides of the body);
- spinal canal;
- articular processes (two);
- transverse processes (two);
- spinous process.

The vertebral body is located in front, and the processes are behind. The latter are the link between the back and the muscles. The flexibility of the spine is developed individually for everyone, and it depends, first of all, on the genetics of a person, and only then - on the level of development.
The vertebra, due to its shape, ideally protects both the spinal cord and the nerves extending from it.
The spine is under the protection of the muscles. Due to their density and location, a layer is formed like a shell. The thorax and organs protect the spine from the front.

This structure of the vertebra was not chosen by nature by chance. It allows you to maintain the health and safety of the spine. In addition, this shape helps keep the vertebrae strong for a long time.
Vertebrae of various departments
The cervical vertebra is small in size and elongated across the shape. In its transverse processes there is a relatively large triangular opening formed by the vertebral arch.

Thoracic vertebra. In his body, large in size, there is a round hole. There is a costal fossa on the transverse process of the thoracic vertebra. Connecting a vertebra to a rib is its main function. There are two more pits on the sides of the vertebra - the lower and the upper, but they are costal.



The lumbar vertebra has a large bean-shaped body. The spinous processes are located horizontally. There are small gaps between them. The spinal canal of the lumbar vertebra is relatively small.

The sacral vertebra. As a separate vertebra, it exists until about 25 years old, then it fuses with others. As a result, one bone is formed - the sacrum, which has a triangular shape, the top of which is turned down. This vertebra has a small free space reserved for the spinal canal. The fused vertebrae do not stop performing their functions. The first vertebra of this department connects the sacrum with the fifth lumbar vertebra. The apex is the fifth vertebra. It connects the sacrum and the coccyx. The remaining three vertebrae form the surfaces of the pelvis: anterior, posterior and lateral.


The vertebra at the coccyx is oval. It hardens late, which compromises the integrity of the coccyx, since at an early age it can be damaged as a result of a blow or injury. At the first coccygeal vertebra, the body is equipped with outgrowths, which are rudiments. In the upper part of the first vertebra of the coccygeal section, the processes of the joints are located. They are called coccygeal horns. They connect with the horns located in the sacrum.
If you want to know in more detail the structure, and also consider what each vertebra is responsible for, you can read an article about this on our portal.


Features of the structure of certain vertebrae
The atlas consists of anterior and posterior arches joined together by lateral masses. It turns out that the atlas has a ring instead of a body. Branches are absent. Atlas connects the spine and skull thanks to the occipital bone. The lateral thickenings have two articular surfaces. The upper surface is oval, joins the occipital bone. The lower round surface connects to the second cervical vertebra.

The second cervical vertebra (axis or epistrophy) has a large process that resembles a tooth in shape. This offshoot is part of Atlanta. This tooth is the axis. Atlas and the head revolve around it. That is why the epistrophy is called axial.

Due to the joint functioning of the first two vertebrae, a person is able to move his head in different directions without experiencing problems.
The sixth cervical vertebra is distinguished by costal processes, which are considered vestigial. It is called protruding because its spinous process is longer than that of other vertebrae.

If you want to learn more and also consider the functions of bends, you can read an article about this on our portal.
Diagnosis of diseases of the spine
Vertebrology is a modern branch of medicine in which attention is paid to the diagnosis and treatment of the spine.
Previously, this was done by a neuropathologist, and if the case was severe, then an orthopedist. In modern medicine, doctors trained in the field of spinal pathologies do this.
Today's medicine provides doctors with numerous opportunities for diagnosing diseases of the spine and treating them. Among them, minimally invasive methods are popular, because with minimal intervention in the body, a greater result is achieved.
In vertebrology, diagnostic methods that are able to produce results in the form of images or other types of visualization are of decisive importance. Previously, the doctor could only prescribe an x-ray.

There are now many more options that can provide accurate results. These include:
- CT scan;
- myelography;
- electroneurography;
- electromyography.
Moreover, today in medical practice, vertebrologists often use a map of segmental innervation. It allows you to associate the cause and symptoms with which vertebra is affected and which organs it is associated with.
Table No. 2. Map of segmental innervation
| Place | Connection | Cause | Symptoms |
|---|---|---|---|
| The organs of hearing and vision, the speech apparatus and the brain | muscle strain | Headaches | |
| seventh cervical vertebra | Thyroid | Hump at the bottom of the neck | Sudden changes in blood pressure |
| The seventh cervical vertebra and the first three thoracic | A heart | Arrhythmia, angina pectoris | Heart pain, palpitations |
| Thoracic vertebrae (fourth to eighth) | Gastrointestinal tract | Pancreatitis, ulcer, gastritis | Heaviness in the chest, nausea, vomiting, flatulence |
| Thoracic vertebrae (ninth to twelfth) | urinary system | Pyelonephritis, cystitis, urolithiasis | Chest pain, urinary discomfort, muscle aches |
| Bottom of the lumbar | Colon | Intestinal dysbacteriosis | Lower back pain |
| Upper lumbar | Sex organs | Vaginitis, cervicitis (in women), urethritis, prostatitis (in men) | Feelings of discomfort and pain |


Anatomy in Chinese
Even several thousand years before mankind invented radiography, Chinese doctors already knew about the connection between the internal organs of a person and the spine.
Based on the theory of acupuncture, the main knowledge that we received from the ancient Chinese is the knowledge of bioactive points that have a direct effect on the internal organs. These points are located near the spine.

Depending on the localization of pain, we can talk about the disease itself. To get rid of it, you need to act on the sore point. This can be achieved with the help of hands (massage) or various means (for example, special needles).

Video - Acupuncture
The ideas of Chinese physicians of that time about the connection between internal organs and vertebrae are completely similar to the map of segmental innervation, which modern doctors have.
Moreover, Chinese scientists in ancient times came to the conclusion that emotions affect the physical state. They were able to create a system for identifying diseases based on emotions. The main emphasis is on which emotional component harms a particular organ.
Table No. 3. Chinese health map.
| Place | Body(s) | Symptoms | Emotion as the root cause |
|---|---|---|---|
| Third thoracic vertebra | Lungs | Respiratory disorders | Sadness |
| fourth and fifth thoracic vertebrae | A heart | Pain | Rage, aggression |
| Ninth and tenth thoracic vertebrae | Liver and gallbladder | Discomfort and pain | Anger, bitterness |
| eleventh thoracic vertebra | Spleen | Performance deterioration | Doubt, oppression, depression |
| Second lumbar vertebra | kidneys | Functional disruption | Fear |
Modern medicine on scientific basis fully confirms all the knowledge that the Chinese scientists of ancient times shared with us.
Treatment
Physiotherapy devices
There are many options for the treatment of the spine, which are carried out in stationary conditions. However, besides them, there is a simple and affordable way of healing - this is oriental massage. Everyone can master it and do it at home.

According to Chinese tradition, human bioactive points are located not far from the above vertebrae (see table No. 2). The distance is two fingers.
At a distance of four fingers are the points where, according to Chinese doctors, destructive emotions accumulate. Walking along the entire length of the spine with just the tips of your fingers, the massage therapist improves the functioning of the whole organism.
Movements are done gently along the spine. You need to move from the highest point down.
The main rule of massage. The person being massaged should enjoy the process and not experience pain. If pain occurs when you press on any point, then you need to ease the pressure.
A simple massage, when performed correctly, can improve the condition of the human body. But the main thing is to get rid of the causes that cause negative emotions. After all, they are usually the root cause of all problems.
Video - Oriental massage Yumeiho
Theory - clinics in Moscow
Choose among the best clinics by reviews and the best price and make an appointment
Theory - specialists in Moscow
Choose among the best specialists by reviews and the best price and make an appointment
Back pain can be experienced not only by the elderly, but also by teenagers and even infants. This pain can be caused by many reasons: both fatigue and all kinds of diseases that could develop over time or be from birth.
In order to better understand where pain sensations come from and what they can mean, as well as to know how to get rid of them correctly, information about the structure of the spine, its departments and functions will help. In the article we will consider the anatomy of this department, we will tell in detail what functions the spine performs and how to keep it healthy.
The spinal column has an S-shape, due to which it has elasticity - therefore, a person is able to take various postures, bend down, turn around, and so on. If the intervertebral discs did not consist of cartilaginous tissue, which is capable of being flexible, then the person would be constantly fixed in one position.
The shape of the spine and its structure ensure balance and upright posture. The entire human body, its limbs and head “holds” on the spinal column.

The spine is a chain of vertebrae articulated by intervertebral discs. The number of vertebrae varies from 32 to 34 - it all depends on individual development.
Departments of the spine
The spinal column is divided into five sections:
| Name | Description | Image |
|---|---|---|
| cervical | It consists of seven vertebrae. It is the most mobile, because a person constantly makes all kinds of movements, turns and tilts of the neck and head. This department itself is shaped like the letter "C", and the convex side faces forward. Blood vessels pass through the transverse processes of the cervical vertebrae, providing blood supply to the brain and cerebellum. If any damage occurs in the cervical region, for example, hernias or fractures, naturally, blood circulation in this area is severely disturbed, and brain cells can die due to insufficient supply of blood and other nutrients, a person may lose spatial orientation (because in the area the head is the vestibular apparatus), suffer from severe headaches, and in his eyes often appear "goosebumps". The upper cervical vertebrae, called Atlant and Axis, are somewhat different in structure from all others. The first does not have a vertebral body, but consists of anterior and posterior arches, which are connected by thickenings consisting of bone tissue. The second is distinguished by a special bone process, which is called the odontoid. Thanks to him, the entire cervical region can be flexible so that a person can turn his head. | |
| Thoracic | Consists of 12 vertebrae where the ribs are attached to form a complete ribcage. It is in this area that most of the main internal organs are located, and therefore the thoracic region is practically motionless. Despite this, it is possible to damage it, and this is very dangerous: along with this, other body systems can also be damaged. The bodies of the vertebrae tend to increase, since they are subjected to some load - this is due to the location of the organs and breathing. Also, the vertebrae in this section are distinguished by the fact that they have special costal half-holes (two for each), into which the ribs themselves “enter”. Outwardly, this department also resembles the letter "C", but, unlike the cervical, it is convex back. | |
| Lumbar | Consists of five vertebrae. Despite the fact that the department is rather small, it performs the most important functions in the entire musculoskeletal system, namely, it takes almost all the load that is placed on the body. And the vertebrae here are the largest. True, it also happens when a certain pathology occurs - lumbarization, in which a sixth vertebra appears in the lumbar region of a person, which does not carry any benefit, but does not interfere with normal life. The lumbar region has a physiological lordosis - this is a slight normal bend forward. If it exceeds the permissible norm, then the person suffers from some kind of disease. It is the lumbar region that is most responsible for the mobility of the legs, while experiencing the load from the upper half of the body. Therefore, you should be extremely careful when performing any physical exercises or lifting weights, because if this is done incorrectly, it is the lumbar region that will suffer - the intervertebral discs begin to “wear out” in it, which leads to hernias that so often occur in this area. | |
| sacral department | Consists of five vertebrae that fuse and form into a triangular bone. It performs the function of connecting the upper part of the spinal column with the pelvic bone. True, they do not grow together immediately, but only by the age of 25 - in infants and adolescents, the sacral section still has some mobility, and therefore it is vulnerable to injury. The sacrum has several openings through which nerve tissues pass, due to which nervous “sensitivity” is possessed bladder, rectum and lower extremities. | |
| coccygeal department | Consists of three or five vertebrae - depending on individual characteristics. In fact, it is rudimentary, but at the same time it performs a number of important functions. For example, in women, it is mobile, which helps in carrying a baby and during childbirth. In all people, it is a link for the muscles and ligaments that are involved in the work of the genitourinary system and intestines. The coccyx also regulates the correct extension of the hips and helps to distribute the load correctly, especially when a person is in a sitting position: it is the coccyx that allows the spine not to collapse when a person is sitting, although the load on his spine is huge. If the coccygeal department did not “take over” part of it for itself, the spine would be easily injured. |
Video - A visual representation of the structure of the spine
Functions of the spine
The spinal column has several functions:
- Support function. The spinal column is the support for all limbs and the head, and it is on it that the greatest pressure of the whole body is exerted. support function discs and ligaments also perform, but the spine takes on the largest weight - about 2/3 of the total. This weight he moves to the legs and pelvis. Thanks to the spine, everything is combined into one whole: the head, and the chest, and the upper and lower limbs, as well as the shoulder girdle.
- Protective function. The spine performs the most important function - it protects the spinal cord from various injuries. It is the "control center", which ensures the proper functioning of the muscles and skeleton. The spinal cord is under the strongest protection: it is surrounded by three bone membranes, reinforced with ligaments and cartilage tissue. The spinal cord controls the work of the nerve fibers that depart from it, so we can say that each vertebra is responsible for the work of a certain part of the body. This system is very well-coordinated, and if any of its components is violated, the consequences will reverberate in other areas of the human body.

- motor function. Thanks to the elastic cartilaginous intervertebral discs located between the vertebrae, a person has the ability to move and turn in any direction.
- damping function. The spine, due to its curvature, dampens the dynamic loads on the body when walking, jumping or traveling in transport. Thanks to such depreciation, the spinal column creates pressure opposite to the support, and the human body does not suffer. Muscles also play an important role: if they are in a developed state (for example, thanks to regular sports or physical education), then the spine experiences less pressure.
Prices for orthopedic shoes
Detailed structure of the vertebrae
The vertebrae have a complex structure, while in different parts of the spine they may differ.
If you want to know in more detail what their functions are, you can read an article about it on our portal.
The vertebra consists of a bony bar, composed of an internal spongy substance, and an external substance, which is a lamellar bone tissue.
Each substance has its own function. Spongy substance is responsible for strength and good resistance, and compact, external, is elastic and allows the spine to withstand various loads. Inside the vertebra itself is the red brain, which is responsible for blood formation. Bone tissue is constantly renewed, due to which it does not lose strength for many years. If the metabolism is established in the body, then there are no problems with the musculoskeletal system. And when a person is constantly engaged in moderate physical activity, tissue renewal occurs more rapidly than with a sedentary lifestyle - this is also a guarantee of spinal health.

The structure of the vertebra
The vertebra consists of the following elements:
- vertebral body;
- legs, which are located on both sides of the vertebra;
- two transverse and four articular processes;
- spinous process;
- the spinal canal, in which the spinal cord is located;
- vertebral arches.
The vertebral body is in front. The part on which the processes are located is behind. The back muscles are attached to them - thanks to them, the spine can bend and not collapse. In order for the vertebrae to be mobile and not rub against each other, intervertebral discs are located between them, which consist of cartilage tissue.
The spinal canal, which is a conductor for the spinal cord, is made up of vertebral foramina, which are created by the arches of the vertebrae attached to them from behind. They are necessary in order for the spinal cord to be as protected as possible. It stretches from the very first vertebra to the middle of the lumbar region, and then the nerve roots extend from it, which also need protection. There are 31 such roots in total, and they spread throughout the body, which provides the body with sensitivity in all departments.

The arc is the basis for all processes. The spinous processes extend backward from the arch and serve to limit the range of motion and protect the spine. The transverse processes are located on the sides of the arc. They have special openings through which veins and arteries pass. The articular processes are located two above and below the vertebral arch, and are necessary for the proper functioning of the intervertebral discs.
It is organized in such a way that the veins and arteries passing in the region of the spine, and most importantly, the spinal cord and all the nerve endings extending from it, are protected as much as possible. To do this, they are in such a dense bone shell, which is not easy to destroy. Nature has done everything to protect the vital parts of the body, and man can only keep the spine intact.
Prices for orthopedic corsets and posture correctors
What are intervertebral discs?
Intervertebral discs are made up of three main parts:
- fibrous ring. This is a bone formation, consisting of many layers of plates, which are connected using collagen fibers. It is this structure that provides it with the highest strength. However, with impaired metabolism or insufficient mobility, tissues can become thinner, and if strong pressure is applied to the spine, the annulus fibrosus is destroyed, which leads to various diseases. It also provides communication with neighboring vertebrae and prevents their displacement.
- Pulpous nucleus. It is located inside the fibrous ring, which tightly surrounds it. The core is a formation similar in structure to jelly. It helps the spine withstand pressure and supplies it with all the nutrients and fluid it needs. Also, the nucleus pulposus creates additional shock absorption due to its function of absorbing and releasing fluid.
With the destruction of the fibrous ring, the nucleus can protrude - such a process in medicine is called an intervertebral hernia. A person experiences severe pain, because the protruding fragment presses on the nerve processes passing nearby. The symptoms and consequences of a hernia are described in detail in other publications. - The disc is covered from below and from above end plates, which provide additional strength and resilience.

If the intervertebral disc is destroyed in any way, then the ligaments located next to the spine and included in the spinal segment try in every possible way to compensate for the malfunction - a protective function is triggered. Because of this, hypertrophy of the ligaments develops, which can lead to compression of the nerve processes and the spinal cord. This condition is called spinal stenosis, and the only way to get rid of it is through surgical treatment.
Facet joints
Between the vertebrae, in addition to the intervertebral discs, there are also facet joints. Otherwise, they are called arcuate. Neighboring vertebrae are connected using two such joints - they lie on both sides of the vertebral arch. The cartilage of the facet joint is very smooth, thanks to which the friction of the vertebrae is significantly reduced, and this neutralizes the possibility of injury. The facet joint includes in its structure the meniscoid - these are processes enclosed in the joint capsule. The meniscoid is the conductor of blood vessels and nerve endings.

Facet joints produce a special fluid that nourishes both the joint itself and the intervertebral disc, and also “lubricates” them. It's called synovial.
Thanks to such a complex system, the vertebrae can move freely. If the facet joints are destroyed, then the vertebrae will come together and undergo abrasion. Therefore, the importance of these articular formations is difficult to overestimate.
Possible diseases
The structure and structure of the spine is very complex, and if at least something in it stops working correctly, then all this affects the health of the whole organism. There are many different diseases that can occur in the spine.
| Name | Image | Description |
|---|---|---|
| Otherwise, this disease is called ankylosing spondylitis. Due to an infection or antigen activation in a person, the intervertebral joints become inflamed, and with the development of the disease, the entire spine gradually begins to become covered with calcium growths, which eventually become hard bone tissue. A person becomes as if "chained" in bone chains, because of which he cannot take any position - he has to constantly be in a bent position. Most often, this disease occurs in men, but it also occurs in women. You can read more about this disease at the link indicated in the first column. |
||
| An intervertebral hernia can form for various reasons: for example, due to excessive overexertion, or vice versa - due to a sedentary lifestyle in the absence of moderate physical activity. It can occur in a person of absolutely any age. A spinal hernia is a nucleus pulposus protruding from the annulus fibrosus. You can also get rid of it by a non-surgical method - you can read more about the treatment at the link indicated in the first column. |
||
| This disease is not very common, however, unfortunately, it is one of the most dangerous. Spinal cancer can manifest itself in different forms depending on where it occurs. If it is detected in time and treatment is started, then it will be possible to get rid of it without surgery and with minimal health losses. No one is immune from such a disease, but if preventive measures are taken, the risk of getting cancer is significantly reduced. You can read about what can be done to cure such a disease or avoid it in the article, the link to which is in the first column. |
||
| Osteochondrosis | Osteochondrosis is one of the most common diseases. It most often occurs in people over the age of 35. Symptoms of it are observed in 9 out of 10 people. Fortunately, you can get rid of such a disease quite simply, and if you do it as quickly as possible, then there will be no unpleasant consequences. And to avoid it, it is enough to avoid a sedentary lifestyle and engage in physical education as often as possible - of course, in moderate doses. Osteochondrosis is characterized by discomfort in the back, impaired posture, weakness and some loss of sensation. |
|
| Osteoporosis | Chronic bone disease, which is characterized by increased fragility of bones. Consequently, patients suffering from osteoporosis are more at risk of various fractures and spinal injuries. It appears due to a lack of calcium, deterioration of metabolism and a sedentary lifestyle. In a patient with osteoporosis, a fracture can occur even from a minor injury, such as a fall or a sharp turn. Very often, people live with osteoporosis and do not even suspect that they have such a disease, since its symptoms are quite common: fatigue, occasional back pain, and problems with nails and teeth. Treatment of osteoporosis can be special physical exercises and taking vitamins and medicines. |
Spine Health
Reading about numerous diseases, people ask themselves: how to keep your spine healthy? For this, there are certain preventive measures that are advised to adhere to people of any age.
- Take care of your posture: for this you can walk for 5-10 minutes a day with a book on your head, and outside the home just control the position of your back. You can set yourself a reminder on your smartphone in order to never forget about a straight back.
- Exercise. Going to the gym a couple of times a week or exercising at home will be beneficial if done correctly and in moderation.

- Watch your weight. Excess weight creates a strong load on the spine, and, in addition, brings a lot of other problems. It is better to get rid of it in time and control nutrition.
- Follow the removal of toxins. To do this, you need to drink plenty of water, as well as eat right. Due to the accumulation of toxins, the metabolism can slow down, which will lead to diseases of the spine.
- Avoid unnecessary weight lifting. It's best not to carry heavy objects unless you're prepared to do so.
Prices for belts for the back
Summing up
The structure of the spine is the most complex formation. Nature created musculoskeletal system so that all important parts of the body are protected. It remains for a person to maintain the health of the spine throughout life.
If you want to know in more detail, namely the lumbar region, you can read an article about this on our portal.
Diagnostics - clinics in Moscow
Choose among the best clinics by reviews and the best price and make an appointment
Diagnostics - specialists in Moscow
Choose among the best specialists by reviews and the best price and make an appointment
The main function of the spine is support, which allows to ensure the rigidity of the skeleton and maintain the usual shape of the body. Therefore, the spine is strong, has a certain flexibility that ensures the balance of the body, and has four natural curves (physiological curves) that act like a spring, which soften sharp vertical loads on the spine (jumping, etc.), allow you to respond to weight-related stresses body and its movements, as well as absorb shocks and shocks while walking. The bends facing the bulge forward are called lordosis (cervical and lumbar), and the bends facing the bulge back are called kyphosis (thoracic and sacral). Kyphosis is the primary curve present at birth. Lordosis - secondary bends that form as the spine grows. Physiological curves can be deformed due to illness or poor posture associated with a weak muscle corset and lack of maintenance of back muscle tone, so the spine begins to work poorly, muscles and ligaments become overly stretched or compressed, and the vertebrae and their joints begin to wear out, in The result is back pain.
Normal spine: rear view, side view
Scoliosis is a genetically determined disease of the musculoskeletal system, characterized by lateral curvature of the spine (in the frontal plane), with twisting of the vertebrae during their growth (it is a pathological condition). Scoliosis can be congenital or acquired.
Causes of scoliosis (most cases of scoliosis occur for reasons that are not entirely clear):
- congenital scoliosis (improper development of the vertebrae) is associated with congenital disorders in the structure of connective tissues with a weakening of the ligamentous structures in all body systems, i.e. the ligaments designed to hold the spinal column upright are too weak to do so. Congenital (primary, hereditary) scoliosis may be accompanied by various congenital changes: developmental disorders (dysplasia) of the hip joints, maxillofacial anomalies (bifurcation of the lips, nonunion of the hard palate), flat feet, anomalies of the biliary and urinary tract.
- Acquired scoliosis occurs most often in children (idiopathic juvenile scoliosis) between the ages of 5 and 15 years (due to poor posture) as the child learns to hold his head and sit, especially in schoolchildren, which is facilitated by incorrect posture during training sessions, which leads to an uneven load on the spine and back muscles, tires and weakens them. In the future, there are changes in the ligaments of the spine and the shape of the vertebrae themselves. Also, scoliosis in children can be a consequence of rickets.
Scoliosis in adults can develop as a result of prolonged asymmetric loads on the back muscles (the so-called professional scoliosis of violinists, seamstresses, porters, etc.). In these cases, the curvature develops slowly and rarely reaches such a degree as in childhood and adolescence. Scoliosis can also be the result of congenital metabolic disorders, the result of lesions in certain diseases, accompanied by the destruction of the lateral sections of the vertebral bodies over a greater or lesser extent, for example, in tuberculous spondylitis, tumors, osteoporosis, degenerative disc disease (osteoarthritis), etc. In patients with damage to the spine and spinal cord, curvature of the spine may occur due to paralysis of the muscles of the back (paralytic form of scoliosis). And the so-called functional scoliosis can occur if the patient has one shortened leg.

Kyphosis can be arched, when one or another section of the spine is evenly curved backwards, and angular, when the spine is sharply curved in a small area (in the region of several vertebrae). Arcuate kyphosis occurs mainly in the thoracic spine (the so-called round back). The reasons for the development of the arcuate form of kyphosis can be congenital weakness of the back muscles, severe rickets suffered in childhood, a long bent position of the body (behind the machine, at the desk, etc.). The presence of arched kyphosis not only violates the posture of a person, but also leads to a decrease in the respiratory capacity of the chest (since a full breath requires maximum extension of the spine), and respiratory failure can adversely affect blood circulation. Often, with arched kyphosis, shoulders pushed forward and lowered down, a protruding or somewhat sagging abdomen are observed. Angular kyphosis occurs predominantly in the thoracic spine and in this case is called a hump. The cause is most often the defeat of the vertebrae by the tuberculous process (spondylitis) and their flattening under the weight of the overlying parts of the body, which is accompanied by a pronounced shortening of the body and a sharp protrusion of the chest. This deformation seriously affects the function of internal organs, work and personal life of the patient.

Lordosis is usually observed in the lumbar spine. Most often, it develops with congenital dislocations in the hip joints, in which the center of gravity of the body in its vertical position is transferred anteriorly and, in order to maintain balance, the body deviates back, bending at the waist. Physiological lumbar lordosis may increase with excessive deposition of fat on the abdomen.
Lordosis is manifested by deformation of the spine and pain due to redistribution of the load on the vertebral bodies and overstretching of the musculoskeletal apparatus of the spine. Active movements of the affected spine are limited. Lordosis is often accompanied by prolapse of the internal organs (stomach, intestines, kidneys), which explains various disturbances in their work.
SPINE [columna vertebralis(PNA, JNA, BNA); syn. spinal column] - the main part of the skeleton of the body, serves as an organ of support and movement, a receptacle for the spinal cord. The spine consists of 32-33 vertebrae, which are conditionally combined into sections (segments) - cervical (C), thoracic (Th), lumbar (L), sacral (S), coccygeal (Co) (printing. Fig.). The spine creates support for the body, being a place of attachment of muscles, takes part in the movements of the body. The vertebrae are connected to each other in different parts of the spine with the help of discontinuous and continuous connections, which ensures greater stability of the spine, on the one hand, and sufficient mobility, on the other.
Comparative anatomy
The phylogenetically initial form of the Spine is the notochord (dorsal string) - a cell strand of entomesodermal origin. As a permanent organ, the notochord exists only in certain lower vertebrates. In most adult vertebrates, the notochord is preserved inside the vertebrae (in fish), in the vertebral bodies (in amphibians), and in the form of a gelatinous nucleus of intervertebral discs (in mammals). In selachia, cartilaginous bodies of the vertebrae are formed in the notochord, in whole-headed and bibreathers, ring-shaped calcareous deposits are formed. The spine of fish is divided into the trunk and tail sections. Starting with amphibians, the cervical and sacral sections are differentiated, between which the thoracic (trunk) remains. The number of vertebrae can vary, reaching 400 in legless lizards and snakes.
In birds, the trunk section of the P. is immobile due to the fusion of the vertebrae with each other, the cervical section is elongated and very mobile; the sacral section consists of a large number of fused vertebrae. In mammals, the P. has the most differentiated structure, including 6–9 cervical, 9–24 thoracic, 1–10 sacral, and 3–46 coccygeal vertebrae.
Embryology
The human spine in its development goes through the membranous, cartilaginous and bone stages. According to N. V. Popova-Latkina, P.'s elements appear in an embryo 7 mm long. The notochord and segments (21 in number) are well identified at this stage of development. In an embryo 9 mm long, the anlages of the vertebral bodies are far apart, separated by layers of the embryonic mesenchyme. When the embryo is 13.5 mm long, the arches of the vertebrae are clearly expressed, and the transverse and articular processes begin to form. The p. of embryos 18–25 mm long has a uniform dorsal curvature with a ventral curvature of the last coccygeal vertebrae. Differences inherent in the vertebrae of different departments are revealed. In embryos 33-37 mm, the P. is curved to a lesser extent than at the previous stage. The vertebrae are almost completely differentiated (spinous processes are still absent). The notochord is reduced and is preserved only in the form of the nucleus pulposus of the intervertebral discs. A characteristic feature of P. in the early stages of development is the similarity of the vertebral bodies in their shape. At the end of the 2nd month intrauterine development sharply increase in the size of the body of the cervical vertebrae. In late-age embryos and fetuses, the Th12 and L1 vertebral bodies are the largest. An increase in the bodies of the lumbar and sacral vertebrae is not observed even in newborns due to the absence of intrauterine graviostatic effects. The laying of the longitudinal ligaments of the P. occurs in embryos 17-19 mm long on the dorsal surface of the vertebral bodies. Intervertebral discs in embryos 10-13 mm long consist of mesenchyme. In embryos 16-21 mm long, fibrous connective tissue develops along the periphery of the disc. Inward from it, a perichordal zone arises, where hyaline cartilage begins to develop around the notochord. P.'s chondrification begins on the 5th - 7th week, and ossification - on the 10th - 12th week. Ossification centers appear first in the lower thoracic and upper lumbar vertebrae, then can be traced in other departments (later in the coccygeal). Each vertebra has three primary ossification nuclei - one in the body and one in each half of the arch. They grow together only by the third year of life. Secondary centers appear along the edges of the vertebral body at 6-8 years in girls and 7-9 years in boys. Their fusion with the vertebral body occurs after 20 years. The sacral vertebrae fuse into a single bone - the sacrum - at the age of 17-25.
Age-related changes Accelerated P.'s growth in length with the achievement of 30-34% of the final size occurs from birth to 3 years. In girls, the thoracic region increases most intensively, then the lumbar and cervical. In boys, the lumbar and thoracic regions grow equally intensively. From 3 to 7 years, P.'s growth slows down. Growth activation again occurs before the onset of puberty.
By the time of birth, P. has a uniform and slight dorsal curvature, although even then mild lordosis (see) and kyphosis (see) are differentiated in it. Changes in the shape of P. after birth are associated with the development of motor skills. When the child begins to hold his head, his cervical lordosis is fixed. The acquisition of the ability to sit, stand and walk forms lumbar lordosis. At the same time, thoracic and sacral kyphosis intensifies. Thus, already in the first year of life, all four P.'s bends in the sagittal plane are indicated. The presence of bends significantly increases the strength of P., since it determines its spring properties.
A change in the shape of P. during aging is manifested by an increase in the curvature of the upper thoracic region, leading to stoop (senile kyphosis). P.'s degenerative changes appear after 20 years. The weakening of the ligamentous apparatus leads to the expansion of the intervertebral spaces and the displacement of individual vertebrae. Ruptures of the annulus lead to the insertion of the nucleus pulposus into the vertebral body, which is often seen in macerated vertebrae. The places of attachment of the fibers of the anterior longitudinal ligament are calcified, which leads to the formation of osteophytes (see). Age-related osteoporosis (see) is clearly manifested in P. after 50-60 years.
Anatomy
Each vertebra (vertebra), except for the I cervical, consists of a body, an arc and processes - a spinous, two transverse and four articular (two upper and two lower). The relative size of the constituent parts of the vertebra and their position are not the same in different departments (tsvetn. Fig. 2-6).
I cervical vertebra (C1; atlas) consists of anterior and posterior arches connected by lateral masses (tsvetn. Fig. 1); II cervical vertebra (C2; axis - axial or epistrophy) has a process fused with the body - a tooth facing upward for articulation with the anterior arch of St and the transverse ligament of the atlas. The superior articular processes are located on the vertebral body on the sides of the tooth (tsvetn. Fig. 2).
The rest of the cervical vertebrae (C3-7) have a small body, a bifurcated spinous process at the end, transverse processes pierced by holes, horizontally located articular processes (tsvetn. Fig. 3). The spinous processes are unequal in length. When the head is tilted, the tip of the spinous process is felt on the back surface. In 70% of cases it is C7 (vertebra prominens), in 20% it is C6, in 10% of cases it is Th1
The thoracic vertebrae (vertebrae thoracicae; ThT_Xn) have a large body, tilted down tiled spinous processes, articular processes located in the frontal plane. On the lateral surface of the body there are upper and lower costal fossae, and at the transverse processes - costal fossae of the transverse processes for connection with the tubercles of the ribs (tsvetn. Fig. 5).
Lumbar vertebrae (vertebrae lumbales; L1-5) have a massive body and a horizontally posteriorly facing spinous process enlarged in a vertical size. The articular processes are oriented sagittally (tsvetn. Fig. 6).
The sacral vertebrae (S1-5) in an adult are fused into a single bone - the sacrum (os sacrum). The sacrum has the shape of a pyramid flattened from front to back and curved backwards, with its base facing L5 and its apex facing the coccyx. At the junction of L5 and S1, on the border of lumbar lordosis and sacral kyphosis, an anterior protrusion is formed - a cape (promontorium). The anterior surface of the sacrum is concave and has four pairs of holes; posterior - convex with uneven relief in the form of ridges arising from the fusion of the processes of the sacral vertebrae, also with four pairs of holes (tsvetn. Fig. 7).
The coccyx (os coccygis; Co 1-4) has the shape of a pyramid, with its base facing up towards the sacrum (tsvetn. Fig. 8).
P. withstands a large static and dynamic load, which is reflected in its structure. The massiveness of the vertebral bodies increases from the cervical to the lumbar, and of the latter, L5 is the most massive. In the sacral region, there is a decrease in body size from S1 to S5 by 3.8 times in the sagittal direction, 2 times in diameter and 1.8 times in height. The reduction also includes the remaining parts of S2-5.
In the center of the vertebra between the body and the arch is the vertebral foramen. On the whole spine, these openings, continuing one into the other, form the spinal canal (canalis vertebralis). It contains the spinal cord with membranes.
Between two adjacent vertebrae, intervertebral foramina (foramina intervertebra-lia) are formed, which serve as the exit point for the roots of the spinal nerves. In the cervical region, the largest opening is between C2 and C3, the smallest between C3 and C4; in the chest - the largest between Th7 and Th8, the smallest - between Th2 and Th3.
The vertebrae articulate with each other using various kinds of connections: cartilaginous (intervertebral discs - disci intervertebrales) between the vertebral bodies, connective tissue between the arcs (yellow ligaments - ligg, flava) and processes, bone (synostoses) in the fused sacrum and coccyx, true joints between articular processes. In P. there are 23 intervertebral discs. Their total height reaches V4 of the length of the P. They have the greatest thickness in the lumbar region. Intervertebral discs perform a shock-absorbing function, having in their composition a slightly compressible gelatinous nucleus (nuci, pulposus) and a fibrous ring (annulus fibrosus) that does not allow it to go beyond the disc. Various types of connections provide a combination of stability and mobility functions. The cervical and lumbar regions have the greatest mobility; the mid-thoracic region of the P. is characterized by minimal mobility. The degree of P.'s mobility depends on age, gender, degree of training, and other reasons.
The strength of P.'s structures is different. For vertebrae, the ultimate load is 40-80 kg/cm 2 , for ligaments with a predominance of collagen fibers (eg, anterior longitudinal) - 5-9 kg/mm 2 , with a predominance of elastic fibers (yellow ligament) - 1 kg/mm 2 .
The source of arterial blood supply to the thoracic and lumbar sections of the P. are the intercostal and lumbar arteries, the cervical section - the vertebral, ascending and deep cervical, ascending pharyngeal, external carotid, lower thyroid, thyroid trunk, transverse artery of the neck, subclavian, superior and first intercostal arteries. A vertebra can have up to 5 sources of blood supply. Arterial networks are formed on the outer anterolateral and on the inner surfaces of the vertebral bodies. The intraorgan arteries of the bodies are combined into anterolateral and posterior groups.
The venous outflow pathways are represented by the anterior, posterior and external vertebral plexuses, paravertebral lateral venous tracts formed by the vertebral, deep ascending cervical veins (cervical P.), unpaired and semi-unpaired veins (thoracic), ascending lumbar and lumbar-iliac (lumbar the Department). In the spinal canal there are anterior and posterior internal vertebral venous plexuses (plexus venosi vertebrales interni ant. et post.).
The taking-away limf, P.'s vessels begin from a network limf, capillaries of a periosteum of bodies of vertebrae, arches and shoots, a perichondrium of intervertebral disks. They are sent to regional limf, nodes, different for different departments of P.
The meningeal branches of the spinal nerves, which form the anterior and posterior nerve plexuses, participate in the innervation of the periosteum of the spinal canal. They are dominated by non-fleshy fibers. The largest nerve trunks in the plexuses are characteristic of the upper cervical and upper lumbar vertebrae. Sympathetic trunks serve as a source of sympathetic innervation; 3-7 stems 0.3-0.5 mm thick are suitable for the intervertebral disc.
X-ray anatomy
For X-ray anatomical study, P.'s radiographs (spondylograms) are most often used in frontal and lateral projections. For a more distinct image for the purpose of a detailed study of the intervertebral joints (facet joints, T.) and interarticular sections of the vertebral arches, radiographs are used in oblique projections. On fig. 1 - 3 schemes of roentgenograms of departments of P. in the main projections are presented.
On a direct radiograph of P., the vertebrae with their anatomical details and intervertebral discs are clearly visible in the form of light gaps between the dense shadows of the vertebral bodies. The latter in an adult have the form of bone density quadrangles with clear, even contours along the upper and lower edges and somewhat concave along the lateral surfaces. As you move away from the cervical to the lumbar, the vertebrae become more massive, and their bodies are higher. In the region of the vertebral bodies along the midline, shadows of the spinous processes are visible. In this case, the spinous process projecting onto this vertebra belongs to the superior vertebra, and only the spinous processes of the lower lumbar vertebrae are projected onto their bodies. In the lateral sections of the vertebral bodies, oval shadows of the legs of the arches are visible, and above and below them are the shadows of the upper and lower articular processes.
On the lateral radiograph, the vertebral bodies, their upper, lower, anterior and posterior contours, as well as articular processes, arches, spinous processes, intervertebral foramina and intervertebral spaces, in which intervertebral discs are located, are clearly visible.
Differences in the anatomical structure of different departments of P. are displayed on radiographs and can be identified by using simple techniques. So, on a direct radiograph of the cervical region of P. (Fig. 1), the upper cervical vertebrae are not detected due to the imposition of a massive shadow of the lower jaw on them. For a clear image of the first two cervical vertebrae, tomography is performed (see) or their radiography in direct posterior projection, directing the central beam of x-ray radiation through the patient's open mouth.
On a direct radiograph of the thoracic P. (Fig. 2), all thoracic vertebrae are displayed, having the form of dense rectangles, on which shadows of the spinous processes and legs of the arcs are projected. On a correctly taken radiograph, the spinous processes are located strictly along the midline of the body. Intervertebral discs in the upper thoracic region of P. are not identified clearly enough, because the plane of the discs due to fiziol, kyphosis of the thoracic region do not coincide with the direction of the central beam of radiation. To obtain a clear image of them, direct radiography of this department of P. is performed with a slight inclination of the radiation beam in the caudocranial direction. In addition to the spinous processes, transverse processes are visible on a direct radiograph, covered by the heads and necks of the articulating ribs.
On the lateral radiograph of the thoracic P., the vertebral bodies and intervertebral discs are displayed more clearly than on a straight line. However, in this case, the upper thoracic region is not clearly identified due to the projection layering of the clavicles and shoulder blades. To eliminate their shadow image, it is recommended to produce a lateral radiograph of this department of P. with the patient in a sitting position with a raised chin and with a girdle of the upper limb displaced downwards and anteriorly.
On a direct radiograph of the lumbar P. (Fig. 3), massive shadows of the vertebral bodies, spinous and transverse processes, pedicles of the arches and intervertebral joints (facet joints, T.) are visible. The vertebrae are separated from each other by wide intervertebral discs, which are more fully reflected in the middle part of the lumbar region, since their projection coincides with the direction of the central radiation beam. Since in this case the intervertebral fissure between the 5th lumbar and 1st sacral vertebrae does not coincide with the central beam of radiation, it is almost invisible. To detect it, a special laying is used, which levels the lumbar lordosis by pulling the lower extremities to the stomach, or radiography is performed with the caudal-cranial direction of the radiation beam. On the lateral radiograph of the lumbar P., the vertebral bodies, intervertebral discs and foramens, articular and spinous processes are clearly identified.
Owing to physiol. curvature of the sacrum and coccyx, a direct radiograph does not clearly reflect all the vertebrae of these departments of the P. Clarity can be made by radiography when the radiation beam is directed at an angle of 25 ° in the cranial direction or a radiograph in a lateral projection.
The final formation of the human spinal column ends by 22-24 years of age. Until this period, the formation of bone elements continues, which is clearly displayed on radiographs. The vertebrae of a newborn on a direct radiograph appear in the form of small oval formations, their height is equal to or even somewhat less than the height of the intervertebral discs, with the exception of the lumbar region, where the bony part of the vertebra is equal in height to the cartilage. In lateral projection, the vertebral bodies also have an oval shape with gaps in the anterior and posterior edges due to the vascular channels. In the future, at the upper and lower edges of the vertebral bodies, stepped impressions formed by cartilaginous rollers are noted, in which ossification points appear by the age of 10-14. Ossified cartilaginous ridges are the apophyses of the vertebral bodies. The substrate for changes in the shape of the vertebrae is the ossification of the apophyses of the vertebral bodies that continues with age, the gradual fusion of the arches with the bodies of the vertebrae, the formation of apophyseal ossification nuclei in the spinous and transverse processes. Features rentgenol. pictures of the spine in children must be taken into account in order to avoid errors in x-ray diagnostics.
Research methods
P. is most often examined in connection with complaints of back pain, deformities, and movement restrictions. Patol, signs are result of P.'s disease or arise owing to nek-ry diseases of internals or extremities. Feedback is possible: the first signs of P.'s pathology can be manifested by pain in the limbs or in the region of internal organs, i.e., be of a reflected, radiating nature.
To determine the localization of the pathological focus, it is necessary to know the identification points of P. (Fig. 4).
P.'s survey is carried out in position of the patient standing, sitting and lying, in rest and at the movements. The patient must be completely naked. First of all, attention is paid to violations of the shape of the body: the level of the shoulder girdle, the position of the shoulder blades, the contours of the waist, the line of the spinous processes, etc. By their symmetry or asymmetry, it is determined whether there is a lateral curvature of the P. With a mild curvature, each spinous process can be marked with ink dots , then the line of the spinous processes will be clearly visible, or tilt the patient forward and examine the back, looking from the side of the head along the line of the spinous processes. In this position, the lateral curvature of the spine - scoliosis (if any) is clearly visible, as well as a one-sided paravertebral muscle roller and a costal hump beginning to form. The muscle roller in the lumbar region can also be due to the tilt of the pelvis with different lengths of the legs. In the absence of lateral curvature of the P., a plumb line fixed to the region of the spinous process of the VII cervical vertebra passes along the line of the spinous processes through the intergluteal fold. Then reveal, whether there is no patol, P.'s distortions in the sagittal plane taking into account that normal P. in cervical and lumbar departments has fiziol, lordosis, and in chest department - a kyphosis, and also taking into account a possibility various violations postures, patol, kyphosis and lordosis. Violations of the shape of the spine and torso can be measured using special instruments - scoliograph, kyphoscoliograph, etc. (see Scoliosis).
The palpation and percussion of P. are carried out in position of the patient standing, lying and sitting. By palpating the spinous processes and interspinous spaces, a painful point or area is established. This is helped by percussion of the spinous processes with the tip of the third finger, while the II and IV fingers of the same hand, lying on the sides of the process, feel muscle tension at the moment of greatest pain. With the help of palpation on the sides of the spinous processes (at a distance of 1-1.5 cm), soreness is determined, the edges can be caused by pathology in the intervertebral joints (facet joints, T.), and even more outwards (in the lumbar region by 2- 3 cm) - in the transverse processes. The body of the VI cervical vertebra is palpated anterior to the sternocleidomastoid muscle at the level of the cricoid cartilage, and the upper cervical vertebrae through the back wall of the pharynx. Palpation of the bodies of the lumbar vertebrae in lean subjects is carried out through the abdomen. If there is no suspicion of vertebral destruction, the patient's response to axial load (pressure on the head) and unloading (pulling the head) is checked.

P.'s mobility is examined during flexion, extension, tilts to the sides and rotation. The cervical region of the P. is the most mobile. In case of pathology, its mobility is limited in the corresponding department. To judge P.'s mobility disorders, it is necessary to know the normal amplitude of movements in each department. P.'s bending happens hl. arr. in the cervical, lower thoracic and lumbar regions. The total amplitude of P.'s flexion is approx. 90 °, and the cervical region accounts for 40 °. When flexed, the normal P. forms a smooth arc (Fig. 5, a), while in case of pathology, the corresponding section of the P. does not participate in flexion, for example, lordosis remains in the lumbar region (Fig. 5, b). When examining the amplitude of extension in a standing position, it is very important to fix the pelvis by pressing on it from behind. P.'s extension amplitude is normally equal to approximately 30°. P.'s lateral inclinations are examined with a fixed pelvis, which is achieved when the patient stands with his legs apart by 50-60 cm. With lateral inclinations, the P. deviates to the side by about 60 °. P.'s rotational movements to the sides are possible at 90 °, and only 30 ° fall on the lower thoracic and lumbar sections. The above figures for the amplitude of P.'s movements are averaged for young people and vary depending on the age of the patient and his physical development. Significant information is provided by the study of the patient in the supine position. In a child lying on his stomach, with passive extension of the P., it is possible to identify a painful point in it, and also to determine the presence of rigidity of the muscle that straightens the spine (Fig. 6). Its rigidity can also be determined when the patient is in the supine position (Fig. 7). To do this, the doctor, clasping the legs of the subject in the area ankle joints, lifts them up, while the back does not bend (a symptom of the Marx board). It is important to identify restrictions on mobility or pain during movements in the costovertebral joints. For this, the patient is asked to take a deep breath and at this time the excursion of the ribs is checked. To identify pathology in P., some neurological symptoms are also usually examined (for example, the symptoms of Laset, Wasserman, etc.). The symptoms revealed by means of the listed research methods are the most general and characteristic of the majority of P.
Techniques rentgenol, P.'s researches are diverse and are applied depending on the research purpose. The most simple and available technique, with a cut it is necessary to begin a research of the normal and pathologically changed P., the X-ray analysis in direct, side and slanting projections is. To identify patol, changes in individual vertebrae, sightings, tomography (see), computed tomography (see Computer tomography) are used. To identify possible patol, changes in the intervertebral discs use discography (see), and to study the ligamentous apparatus - ligamentography (see). In order to study the state of the spinal canal, myelography is performed (see). To determine the degree of functional mobility and possible patol, displacement of the vertebrae, lateral radiographs are performed in a state of maximum flexion and extension of the corresponding department of P. (functional radiography). Much less often they resort to a contrast study of blood vessels - venospondylography (see Phlebography), vertebral angiography (SM.).
Pathology
Malformations
According to the morphogenetic classification of V. A. Dyachenko, anomalies in the development of P. are divided into two groups: anomalies of ontogenetic significance and anomalies of phylogenetic significance. The first group includes anomalies in the development of the vertebral bodies (clefts, defects, wedge-shaped vertebrae, platyspondylia, brachyspondylia, etc.), anomalies in the development of the vertebral arches (clefts, underdevelopment, anomalies in the development of the articular processes), as well as congenital synostoses (see). The second group includes os odontoideum, atlas assimilation, cervical ribs, sacralization (see) and lumbarization (see).

Congenital clefts of the vertebrae occur in all departments of P., but more often in the lower lumbar. The cleft of only the arches is called spina bifida (see), and the complete splitting of the vertebra (body and arches) is called rachischisis. Rakhishizis with a median location of the gap may not be accompanied by P.'s deformation; with an asymmetric or oblique arrangement of the fissure, especially in combination with other malformations of the vertebrae in this segment of the P. (for example, with unilateral micro-spondylosis of half of the vertebra, anomaly of the articular processes), a significant deformity of the P. develops (Fig. 8). Often rachischisis, like spina bifida, is accompanied by hypertrichosis (Fig. 9).

Wedge-shaped vertebrae and hemivertebrae can be localized in any department of P., but are usually observed on the border of departments. Lateral wedge-shaped hemivertebrae are more common. A typical wedge-shaped hemivertebra (Fig. 10) consists of a semi-body, a transverse process, and a semi-arch with an articular process. In the thoracic region of P., the hemivertebra bears an additional rib. There are single, double and multiple wedge-shaped hemivertebrae. If two hemivertebrae are located on opposite sides of the P. at different heights (through 2-3 normal vertebrae), they are called alternating (Fig. 11). Since the growth of the vertebrae in height occurs due to the epiphyseal plates (adjacent to the upper and lower surfaces of the vertebral bodies), with a unilateral arrangement of the lateral hemivertebrae, the scoliotic curvature of P. (see Scoliosis) is more pronounced. Even in the presence of one hemivertebra, if it has two epiphyseal plates (“active” hemivertebra according to I. A. Movshovich), P.'s curvature is prone to progression. In the presence of "inactive" hemivertebrae (they have one epiphyseal plate each), P.'s curvature does not progress. This is especially evident in the presence of the so-called. butterfly-shaped vertebra, consisting of one active and the other inactive hemivertebra (Fig. 12). However, the progression of P.'s curvature is associated not only with the activity of the hemivertebra - this process is more complex and is due to a combination of a whole range of factors.
Platyspondylia and brachyspondylia. Platyspondyly is characterized by an expansion of the vertebral body in diameter, and brachyspondyly is characterized by a decrease in its height, flattening and shortening. The combination of these -types of deformation is called "platybrachyspondylia". Such a deformation is characteristic of Calve's disease (see Calve's disease), however, with platibrachispondylia, there is a multiplicity of lesions, the presence of other malformations, and the normal structure of the deformed vertebra. With multiple brachyspondylia, a disproportionate shortening of the trunk is noted.
Malformations of the articular processes, as a rule, are observed in the lumbar and sacral sections of the P. and manifest themselves in the following forms: anomalies in the position of the articular surfaces of the articular processes in relation to the sagittal plane, anomalies in the size of one of the processes, anomalies in the articulation of the articular process with the arch of the adjacent vertebra, the absence articular processes, etc. These anomalies usually do not lead to P.'s deformation, however, they create unfavorable static-dynamic conditions that contribute to the earlier development of osteochondrosis (see) and deforming spondyloarthrosis (see). In a lumbosacral segment of P. a number of malformations meets still. Among them, attention should be paid to spondylolysis and spondylolisthesis (see).

Congenital synostoses (blocking, concretion) of the vertebrae are observed in all departments of the P. They can be complete and partial. With complete synostosis (see), the bodies, arcs and processes of the vertebrae are blocked, with partial synostosis, only the bodies or only the arcs. With complete synostosis, there is no significant deformation of the spine. The partial synostosis causes deformation in the course of P.'s growth, the form a cut depends on localization of a synostosis. So, for example, when blocking only the vertebral bodies, kyphosis develops (Fig. 13). The occurrence of such a deformity is explained in the embryogenesis of the P. The formation of the intervertebral disc occurs in the direction from back to front: at the back of the vertebral bodies at a certain stage of embryonic development are already separated by a formed disk, and in front they still have a common structure. And if at this stage (5-7th week of embryogenesis) the development of P. stops, anterior synostosis of the vertebrae is formed. A typical example of a complete widespread synostosis of the cervical spine is the Klippel-Feil syndrome (see Klippel-Feil disease).
Congenital synostoses of the vertebrae often lead to the development of deforming spondylarthrosis at a relatively early age (see) above and below the blocked vertebrae due to increased functional load.
Os odontoideum - a malformation associated with non-fusion of the ossification point of the odontoid process of the axial vertebra with the body of the latter. This malformation of the P. is a potential cause of instability of the upper part of the cervical P. The absence of a bone connection between the tooth and the body of the axial vertebra in trauma easily leads to transdental dislocation of the atlas (see below Injuries). Very rarely there is a missing tooth.
Assimilation (occipitalization) of the atlas is expressed in the fusion of the atlas with the occipital bone. Possible full and partial merger. Merged can be one or both lateral masses of the vertebra, its arc, while the atlas can be displaced forward or to the side. The deformation can be accompanied by flattening of the atlas, its rotation, and disruption of the shape of the large (occipital) foramen, which creates unfavorable conditions for the medulla oblongata: the tooth of the axial vertebra (C2) when turning the head can have a traumatic effect on it. With incomplete asymmetric occipitalization of the atlas, torticollis is usually observed (see), which in this case is attributed to the bone form of this pathology.
Cervical ribs are a rare malformation. Usually they are combined with other malformations. More often they are associated with the VII cervical vertebra. They can range in size from a slightly pronounced rudimentary formation to well-formed ribs reaching the sternum or soldered with their anterior ends to the 1st ribs. In children, the cervical ribs usually do not manifest themselves, in adults, symptoms of irritation of the brachial plexus and compression of the subclavian artery may appear - pain, paresthesia, muscle hypotrophy of the limb, the pulsation of the arteries on the corresponding arm is weakened. In case of persistent neurovascular disorders, the removal of the rib along with the periosteum is indicated.
At an asymptomatic current of anomalies of development of P. of treatment is not required. With the development of P.'s deformity or complications of malformations (eg, spondylarthrosis), various types of conservative and surgical treatment are used.
Damage
Injuries occur with a different mechanism of action of the traumatic force on the P. Basically, this is flexion, flexion in combination with rotation, extension and compression. Possible isolated damage to the ligaments, most often interspinous and supraspinous, fractures of the bodies, arches, processes of the vertebrae, damage to the intervertebral discs, dislocations or fracture-dislocations of the vertebrae.
Damage to the interspinous and supraspinous ligaments is often observed in combination with a P fracture. Most often it is observed in the cervical, then in the middle and lower thoracic regions.
With isolated damage to the interspinous or supraspinous ligaments of P., localized pain is observed, and when it is combined with a fracture of a vertebra, especially the arch or spinous process, the pain has a radiating character. At the same time, there is a reflex contraction of the muscle that straightens the spine, with a sharp limitation of the mobility of the injured part of the P., in the lumbar region, the "symptom of the reins" is sometimes clearly detected - the tension of this muscle, determined by the eye in the form of rollers on the sides of the spinous processes. On palpation in the area of rupture of the interspinous ligament, pain is determined in the interspinous space, palpation of the spinous processes is slightly painful. When the supraspinous ligament is ruptured, palpation often determines retraction in the area of the interspinous space and divergence of the spinous processes, which is clearly visible on the lateral radiograph. If there is doubt about the presence of a rupture of the interspinous ligaments of P. and provided that other damage to P. is not determined on radiographs, it is possible with great care to resort to functional radiography (lateral radiographs in the position of flexion and extension of P.). For the diagnosis of fresh damage to the interspinous ligaments, the method of ligamentography can be applied (see).
Treatment of isolated injuries of the interspinous and supraspinous ligaments of P. is conservative: novocaine blockade (on the sides of the spinous processes) of the area of damage, bed rest on a bed with a shield. The immobilization of the cervical region of P. is carried out with sand rollers or Glisson's loop with a load of up to 2 kg. Assign physiotherapy, massage, exercise therapy. After the elimination of acute events, wearing a head holder and an extension corset (for the lumbar region) is indicated for 4-6 weeks.
Spinal fractures are severe injuries of the musculoskeletal system and amount to approx. 2-2.5% of all fractures. P.'s fractures often occur as a result of indirect trauma - when falling from a height onto the legs, buttocks, head, and direct injuries - with a direct blow to the back. P.'s fractures can be single and polyfocal (multiple), with and without damage to the spinal cord and spinal nerve roots, with damage to the intervertebral disc (penetrating, according to Ya. L. Tsivyan) and without damaging it. Depending on the lesion of the anatomical component of the vertebra, there are fractures of the body (compression, ringed), arches of the processes of the vertebra. Of significant practical importance is the division of P.'s fractures into stable and unstable. The latter occur with joint damage in the anterior and posterior sections of the vertebra.
Wedge, P.'s fracture manifestations are different - from the complete absence of symptoms in certain types of trauma to severe wedge, pictures: severe pain, intestinal paresis, nevrol, disorders and dysfunction of the pelvic organs in severe fractures of the spine with damage to the spinal cord or spinal roots nerves (see Spinal Cord Injury). The diagnosis of a fracture is made on the basis of studying the mechanism of injury, visual and palpation data, radiography P. With a fresh injury, i.e. before the onset of reparative changes, rentgenol, signs of a compression fracture of the vertebral body are deformation of the latter and increased shadow of the bone substance along the upper its sites. Most often, wedge-shaped flattening is observed with a decrease in the height of the anterior part of the vertebral body in only one lateral projection, while maintaining the normal height of the intervertebral fissure. This deformation may not be accompanied by radiographically documented changes in the structure with minimal depression of the upper horizontal plate. Only the upper plates are pressed in, while the lower ones remain intact. This symptom is the most important in the differential diagnosis of traumatic fractures with patol, compressions and congenital anomalies.
A variant of a compression fracture should be considered a traumatic insertion of a cartilaginous intervertebral disc into the vertebral body - the so-called. traumatic cartilaginous hernia (Fig. 14). The disc is embedded in the cranial plate at its anterior edge. Radiologically, with a slight or completely absent deformation of the vertebral body, a narrowing of the “X-ray intervertebral fissure” is detected (due to the narrowing of the cartilage on the radiograph). The absence of signs in such a traumatic implantation of the intervertebral disc is subsequently replaced by the development of a limited depression of the contour and sclerosis around the prolapsed disc.
Radiographically documented outcomes of P.'s injury depend on the nature of the injury. With a "clean" compression fracture rentgenol, the picture of the affected vertebra immediately after the injury and for a long time later is often the same. At the same time at the ruptures of sheaves and disks accompanying a fracture or a fracture-dislocation, X-ray negative in the early period, after a nek-swarm time appear rentgenol. signs of ossification, calcification, etc. (Fig. 15). In this case, bone blocking of the vertebral bodies, ossification of the ligaments, calcification of the discs, and ankylosis sometimes occur.
In children, fractures and dislocations of the vertebrae account for approximately 0.2% of all types of injuries (N. G. Damier, 1950). Compression fractures of the thoracic vertebrae are more common. Diagnosis of P.'s fracture in children is difficult due to incomplete ossification of the vertebrae, especially in the presence of osteochondropathy of the vertebral bodies. Quite often wedge-shaped deformation of a body of a vertebra, edges at the same time is observed, regard as a compression fracture. In young and middle-aged children, compression fractures of individual vertebrae, with proper treatment, can be completely cured with the restoration of the normal shape and height of the compressed vertebra (Fig. 16).
Rentgenol, signs of compression of the vertebrae in children are: 1) straightening of the horizontal platforms of the vertebral bodies in children aged 6-8 years or concavity at an older age; 2) thickening of horizontal platforms; 3) compaction of the structure of the spongy substance of the compressed vertebrae; 4) an increase in the height of the intervertebral discs in their anterior section compared to normal ones.
In elderly and old people with severe osteoporosis of the vertebrae, compression fractures occur as a result of minor trauma, for example, when falling on the floor and even as a result of shaking while driving a car. Quite often at the same time compression fractures of the vertebrae go unnoticed and are detected by chance during X-ray examination of P. for another reason. In addition, in older people, the vertebral bodies can gradually deform without fracture. Therefore at statement of the diagnosis careful studying of the anamnesis and a wedge, manifestations at the moment of an injury is necessary.
Fractures and dislocations in the cervical spine occur predominantly in young men, most often as a result of indirect trauma, for example, when falling from a height on the head (in divers) or when a weight falls on the head. Dislocations and subluxations of the cervical vertebrae, especially the atlas, often occur as a result of uncoordinated movement of the head, for example, in a passenger with a sudden stop of a car.
In fracture-dislocation, an anatomically complex injury is created, consisting of the following components: 1) a fracture of the body (bodies) of a vertebra of one type or another (compression, compression and marginal detachment, only marginal detachment); 2) rupture of the ligamentous apparatus; 3) disc rupture; 4) dislocation (displacement) of the vertebra in the area of the articular processes (often in combination with a fracture of the articular processes).
Injuries of the I and II cervical vertebrae occupy a special place among other injuries of the cervical region of the P. Anterior displacement of the atlas in transdental or transligamentous dislocation (Fig. 17) can cause instant death due to compression of the spinal cord. Atlas fractures are observed in the form of a fracture of the anterior or posterior arch and in the form of a comminuted or explosive fracture (Jefferson's fracture). If the II cervical vertebra is damaged, the fracture line may pass in the region of the tooth (Fig. 18) or its base (differential diagnosis with os odontoideum is necessary), in the region of the arch plate or its legs (in the latter case, traumatic anterior spondylolisthesis of the II cervical vertebra is possible; such damage called a fracture of the hanged man), marginal fractures of the vertebral body are possible.
Damage to the III-VII cervical vertebrae is characterized by fractures of the bodies, arches, processes, dislocations, subluxations, fracture-dislocations. With a bilateral fracture of the legs of the arches, traumatic spondylolisthesis is possible (see). The fracture that occurs when the head hits the bottom of the reservoir when diving (diver's fracture) is especially severe. Most often, the V-VII cervical vertebrae suffer from this. Due to a sharp flexion of the neck, combined with violence along the vertical axis, a compression comminuted fracture of the vertebral body occurs. Fracture divers are often complicated by paralysis of the limbs and pelvic organs.
Wedge, signs of fractures of the cervical vertebrae: forced position of the head, tension neck muscles, sharp pains when moving the head. In the diagnosis of fractures of the cervical vertebrae, the main role is given to X-ray examination (for I - II cervical vertebrae - always through a wide-open mouth); The tomographic method is also important.
Fractures of the thoracic and lumbar vertebrae most often occur in the lower thoracic and upper lumbar regions, i.e., where the less mobile section passes into the more mobile one. Most often, compression fractures of the vertebral bodies occur with their wedge-shaped deformation, i.e., a decrease in body height in the anterior section. There are three degrees of compression: 1st degree - marginal fractures of the vertebral body without compression or compression with a decrease in the height of the vertebral body to 1/3 of it; 2nd degree - with a decrease in the height of the vertebral body by 1/3 - 1/2; 3rd degree - with a decrease in the height of the vertebral body by more than 1/2. Fractures of the 2nd and 3rd degree can be combined with damage to the intervertebral disc. Less common than compression fractures are comminuted fractures of the vertebral bodies and fracture-dislocations in case of damage in the anterior and posterior sections of the vertebrae. The latest damage is unstable. Various types of typical vertebral fractures are shown in Fig. 19. Immediately after the injury, there is girdle pain, difficulty breathing (in case of a fracture of the thoracic vertebrae), radiating pain in the abdomen (in case of damage to the lumbar vertebrae), local pain on palpation of the spinous processes, muscle tension on the sides of the spinous processes, forced posture of the victim. In case of a fracture of the transverse processes of the lumbar vertebrae, in addition, there is a symptom of a “stuck heel” - the inability to tear a straight leg from the bed and, as a rule, a psoas symptom - a sharp pain in the lumbar region during forced extension of a limb bent at the hip joint. The final diagnosis is established at rentgenol. research.
With a fracture of the lower thoracic or lumbar vertebrae and the resulting retroperitoneal hematoma, patol is possible, manifestations from the abdomen from local pain and mild tension in the abdominal muscles to phenomena resembling acute intraperitoneal bleeding or rupture of a hollow organ - acute abdomen (see), intestinal paresis (cm.). When P.'s fracture is combined with damage to the spinal cord, nevrol develops, disorders of varying degrees (see Spinal cord).
Fractures of the processes of the vertebrae are most often observed in the form of single and multiple detachments of the transverse processes of the lumbar vertebrae. The x-ray shows the downward displacement of the fragment (or fragments) characteristic of a fracture of the transverse process and the absence of cortical substance at the fracture site. The same picture is observed with isolated fractures of the articular processes (which should be distinguished from the sometimes occurring additional ossification nuclei at the tops of the articular processes). Avulsion fractures of the spinous processes (most often in the lower cervical vertebrae, less often in the lumbar) on a direct radiograph are characterized by a downward displacement of the tip of the spinous process. The radiograph in the lateral projection well documents this kind of detachment of the free part of the spinous process. Isolated detachments of the spinous processes of the V lumbar vertebra and the spinous processes of the sacrum are possible with gunshot tangential wounds. Traumatic fracture dislocation with displacement of the vertebra anteriorly or to the side is usually accompanied by fragmentation of the arch, fracture or dislocation of the articular processes, but never gives a picture of spondylolysis typical of non-traumatic displacement.
Fractures of the sacrum and coccyx - see Pelvis, Sacral region, Coccyx.
Treatment of spinal injuries
When providing first aid, it is necessary to lay the victim on a rigid stretcher; in case of a fracture of the thoracic and lumbar sections of the P., it is possible to lie on the stomach. Transportation of the patient in a sitting position is unacceptable. In case of a fracture of the cervical region of P., fixation is carried out with a rigid collar-head holder or a wire splint curved in the shape of the neck, or, finally, with sandbags laid on the sides of the neck, while the patient should lie on his back on a rigid stretcher (see Immobilization).
The nature and timing of treatment depend on the form, localization and degree of damage to P., and the basic principle should be followed - early elimination of displacement, reliable fixation and functional treatment. With rotational subluxation of the atlas, treatment is carried out by traction (see) Glisson's loop (1.5-2 kg) for 2-3 weeks; after removing the traction for the same period, immobilization is prescribed with a Shants collar or a plastic head holder (Fig. 20). For fractures of the I and II cervical vertebrae, treatment is carried out in a cranio-thoracic plaster cast (see Plaster technique). In case of a fracture of the tooth of the II cervical vertebra without displacement or after its simultaneous reduction, plaster immobilization is carried out for 6-8 months. Treatment of dislocation fractures and unstable fractures is carried out by the method of skeletal traction behind the skull with a load of up to 7-8 kg, followed (after 6-8 weeks) by the imposition of a craniothoracic plaster bandage (Fig. 21). Traction with a Glisson loop is ineffective. Nonunion of the odontoid process due to improper treatment leads to the development of atlantoaxial instability, accompanied by trauma to the spinal cord, spinal nerve roots and the development of paralysis. This complication is a direct indication for surgical treatment - decompressive laminectomy (see) with simultaneous spinal fusion (see), more precisely occipitospondylodesis. In case of fractures of the III-VII cervical vertebrae, if there is a slight compression of the body of one or two vertebrae, as well as in case of comminuted fractures of the body without displacement of fragments, in case of fractures of the spinous and articular processes and arches without displacement, treatment is carried out with a Glisson loop (2-3 kg) followed by (after 2-3 weeks) by applying a craniothoracic plaster cast for 2-3 months. In case of dislocation and subluxation of the cervical vertebrae, one-stage reduction is performed with fixation with a plaster cast. However, in cases of unstable reduction, skeletal traction is indicated. If there is a fracture of the vertebral bodies with axial (kyphotic) deformity, a crushed fracture with displacement of fragments, unstable fracture dislocation, as well as nevrol, complications, skeletal traction behind the skull is most effective. With irreducible fracture-dislocations, especially accompanied by nevrol, complications, a stabilizing surgical treatment is shown, with indications - with decompression of the spinal cord.
With a compression fracture of the thoracic and lumbar vertebrae with a slight wedge-shaped deformity of the P., it is necessary to ensure the preservation of lumbar lordosis and full muscle tone. Therefore, it is enough to lay the patient on his back on a bed with a shield, put a small roller under the lumbar region and start treatment as soon as possible. gymnastics. Patients are allowed to walk in a removable corset after 2 months. after injury. With significant compression of the vertebral body in the lower thoracic or lumbar sections of P., reclination is shown by simultaneous (forced) extension of P. after local anesthesia of the vertebrae (Fig. 22) or by gradual extension of P. The latter method is preferable, since it is better tolerated by patients and usually, in contrast to simultaneous reclination, it does not cause intestinal paresis. Gradual reclination of the vertebra can be carried out on the Kaplan reclinator or by stretching on a hammock (Fig. 23): a cloth hammock 15-20 cm wide (with a cotton-gauze lining) is brought under the patient's lower back, the straps are thrown over blocks on two Balkan frames with a transverse crossbar . Reclination is carried out with weights (depending on the weight of the patient), which ensure the formation of lumbar lordosis (shoulder blades and buttocks should not come off the bed). After 2-3 weeks. vertebral reclination is usually achieved. After 2 months the patient is allowed to walk in a corset. A number of surgeons use surgical treatment for compression fractures of the lumbar vertebrae. It allows you to put the patient on his feet early and not prescribe a corset for subsequent treatment. The essence of the method consists in preliminary simultaneous or gradual reclination of the vertebra and internal fixation of the damaged vertebrae and neighboring intact vertebrae behind the spinous processes of P. with wire, special metal clamps, lavsan tape or cord. With multi-comminuted fractures of the vertebral body and with simultaneous damage to the intervertebral disc (penetrating fractures), some surgeons (Ya. L. Tsivyan) suggest immediately performing anterior spinal fusion. In case of a fracture with damage to the spinal cord and roots of the spinal nerves, decompressive surgical treatment, elimination of the cause that caused compression of the spinal cord or roots of the spinal nerves, and fixation of P.
In contrast to the treatment of uncomplicated P. compression fractures in young and middle-aged people, in older people with widespread P. osteoporosis, the affected vertebra should not be reclined, since this creates unfavorable conditions for fracture healing. The patient is placed on a bed with a shield and, after the pain has disappeared, they are allowed to turn around, but do not sit down or stand up. After 1-1.5 months. patients are allowed to walk without a corset. In children, reclination of the vertebrae is well achieved in a plaster bed (see Plaster technique).
Physiotherapy exercises play an important role in the treatment of P.'s injuries; it restores the natural muscular "corset" that is able to keep P. in an upright position and ensures its normal mobility, springing and tolerance to static and dynamic loads.
In persons of young and middle age, with a small degree of compression (a decrease in the height of the vertebral body by no more than 1/3) and a generally satisfactory condition, a functional method of treatment developed by E. F. Dreving is preferable, which consists in unloading P., stretching and systematic application of the treatment. . gymnastics from 2-5 days after injury. With compression fractures of the cervical vertebrae and immobilization with Glisson's loop, a set of exercises is used from light movements of the upper and lower extremities at a slow pace with frequent pauses for rest. Exclude exercises with flexion of the body, turns and tilts of the head. During the period of immobilization with a plaster cast, the motor regime is expanded, the patient is allowed to sit and walk. Apply general developmental exercises for the muscles of the trunk, upper and lower extremities, performed in the prone position, sitting and standing. It is necessary to exclude sharp turns of the torso, head, jumps and jumps. After removing the cast, in addition to general developmental, it is advisable to use exercises that strengthen the muscles of the neck, exercises in balance and coordination of movements. With compression fractures of the thoracic and lumbar vertebrae, in relation to the phases of treatment, the course of exercise therapy should be divided (Fig. 24) into four periods. In period I, approx. 2 weeks in the initial position lying on the back, breathing and general tonic exercises are performed, involving the upper and lower limbs in movements. Stretching during classes is reduced. Exercises are performed at a slow pace 3-6 times for 10-15 minutes. In the II period, which lasts an average of 4 weeks, exercises are used to strengthen the muscles of the back and abdomen, train the vestibular apparatus, and also more active movements for the upper and lower extremities at an average rate of 8-10 times for 20-25 minutes. The transition from one period to another must be strictly individualized in accordance with the patient's condition, gender, age, development of his motor skills. III period lasts an average of 2 weeks. The duration of classes is increased to 30-45 minutes, each exercise is repeated 10-15 times. By the end of this period, with the help of physical exercises, muscle support should be created for P. by significantly strengthening the muscles of the back and abdomen. 7-10 days before the start of walking, it is necessary to include exercises to train the musculo-articular apparatus of the lower extremities in the classes. Except physical exercises, it is necessary to apply to lay down. massage of the muscles of the lower extremities and back. The exercises of the IV period are transferred with a general satisfactory condition of the patient, with a well-developed muscular corset, and the absence of pain (at rest and after exercise) in the area of the fracture. After the patient has adapted to the vertical position, dosed walking should be used, gradually increasing its duration. Continue to treat. massage of the muscles of the back and lower extremities. The restoration of the main functions of P. is more effective during classes in the water. After discharge from the hospital, it is necessary to continue exercise therapy for a long time on an outpatient or sanatorium basis, where adaptation to loads identical to the patient's main activity is gradually restored.
In the elderly, exercise therapy is used to maintain the general tone and functional ability of the muscles, prevent osteoporosis, complications from the internal organs, etc. The volume and duration of classes, as well as the time of bed rest, are reduced in such patients. Throughout the course of treatment, massage of the muscles of the back and abdomen is carried out. and before getting up - massage of the lower extremities. During the period of wearing a corset, the patient continues to engage in exercise therapy in the supine position (without a corset) and standing (in a corset).
With more pronounced compression of the vertebral bodies and ongoing gradual reclination of P. during the first 2 weeks. prescribe exercises to maintain the optimal level of activity of the circulatory, respiratory, digestive, general muscle tone. With permission to roll over on his stomach (with the horizontal position of the reclination bed), the patient performs extension of the body without active participation back muscles by straightening the arms outstretched forward. During this period, in the supine position, he also performs exercises consisting in bending in the thoracic spine, relying on the elbows and raising the pelvis, relying on the legs bent at the knees. In the future, they gradually move on to active exercises that provide more intense tension in the muscles of the back and abdomen, with alternating exercises for the upper and lower extremities. Massage the back muscles. In case of fractures of the transverse and spinous processes of the vertebrae, exercise therapy is carried out according to the method of treating fractures with long-term traction. However, the intensity of the loads and the expansion of the motor regimen are somewhat different: exercises in the prone position can be performed after 4-6 days, on all fours - after 10-15 days, dosed walking and standing exercises - after 3-4 weeks.
In the complex treatment of P.'s injuries, in addition to exercise therapy, great importance has physiotherapy, carried out both during the period of treatment in a hospital, and after discharge.
Physiotherapy for P.'s fractures aims to relieve pain and accelerate the regeneration of damaged tissues. Against the background of anesthesia conditions for effective carrying out to lay down are created. actions, in particular turning over patients from a back on a stomach, wedging of the damaged vertebra on various reclinators, carrying out to lay down. physical education lying on the stomach, accelerating the transfer of patients to a vertical position with or without external immobilization.
In the treatment of patients with stable compression fractures of the P. according to the widely used functional method, when turning from the back to the stomach is allowed from the 2-3rd day after the injury, UV irradiation is used with fields of 150-200 cm 2 along the P. The first field is on the area fracture, the second - below it by 2-3 cm, the third - above the first by 2-3 cm. Irradiation begins with three biodoses, with their subsequent increase (half of the biodose for each field). A total of 12 sessions are carried out (4 for each field). One of the fields is irradiated daily.
Electrophoresis with analgesic mixtures is carried out longitudinally along the P. or paravertebral. You can use 1-5% novocaine solution or Parfenov solution, including cocaine, dicaine 1.5 ml each, adrenaline solution 1: 1000-9 ml, distilled water 450 ml. A simpler mixture of Parfenov consists of 0.5 ml of sovkain, novocaine, adrenaline solution 1: 1000-2.5 ml, distilled water 200 ml. Current strength 12-15 mA, duration of exposure 15-20 minutes. (see Electrophoresis).
From the 4-5th day after the fracture, calcium inductophoresis is applied directly to the area of the injured vertebra. Galvanic electrodes with an area of 150 cm 2 are placed longitudinally: active with 10% solution of calcium chloride - on the fracture area, indifferent - 5-8 cm below it. Strength direct current 8 - 10 ma. The strength of the anode current is 160-180 mA. Impacts are carried out daily for 10-20 minutes; total for the course - 12 impacts. After the very first physiotherapeutic procedures, the expressed pain sensations are significantly reduced, and after the course of treatment they completely disappear. It allows to be engaged in earlier terms to lay down. physical education and introduce physical exercises with a greater range of motion.
A good analgesic effect, which also favorably affects the reparative regeneration of the damaged P., is exerted by a low-frequency (50 Hz) magnetic field generated by the Polus-1 magnetotherapy apparatus. If, due to the nature of P.'s injury, patients cannot be turned on their stomach and they are treated in the supine position, the effects begin on the 2nd day after the injury, installing round inductors with a U-shaped core on the inguinal regions (indirect effect). In the position of the patient on the stomach, the inductors are installed from the back, above and below the injury site. Magnetic field induction 30-35 tl, type of magnetic field sinusoidal or half-wave in continuous mode; per course - 20-25 effects (see Magnetotherapy).
Favorable effect in the recovery period after P.'s fracture has swimming in the pool and underwater douche-massage (see).
To strengthen the muscles of the limbs and torso, electrical stimulation is carried out with the UEI-1, SNIM-1, Amplipulse-3, Amplipulse-4 and Stimulus-1 devices (see Impulse currents). The expressed therapeutic effect renders application in complex treatment of mud therapy (see), hydrogen sulfide, brine and other baths (see).
San.-kur. treatment of patients with uncomplicated P.'s injuries is carried out at the balneological resorts of Pyatigorsk, Nalchik, Archman, Goryachiy Klyuch, Yeysk, Sergievsky Mineralnye Vody, Sochi, Khmelniki, Ust-Kachka, etc., as well as at the mud resorts of Birshtonas, Druskininkai, Yeysk, Krainka, Odessa, Nalchik, etc.
Diseases
From P.'s diseases allocate its deformations, degenerative, inflammatory and infectious diseases and tumors.
Deformities of the spine are conditionally divided into curvature in the anteroposterior and lateral directions. The first type includes kyphotic curvatures (see. Kyphosis), curvatures arising from osteochondropathy of the vertebral bodies (see Calve's disease), curvature with osteochondropathy of the apophyses of the vertebral bodies (see Scheuermann-Mau disease), Kyummell's disease (see Kyummell's disease). Kyphosis develops as a result of P.'s inflammatory diseases (see Spondylitis) with their untimely treatment, with dystrophic diseases, and tumors. Lateral deformation of P., to be exact combined with a torsion of vertebrae, represents scoliosis (see).
Degenerative diseases of the spine - intervertebral osteochondrosis (see), sometimes called discopathy, discosis (see), deforming Spondylarthrosis (see), spondylosis (see), Bostrup's disease.
Conservative treatment in the form of thermal and other physiotherapy procedures (see above) often leads to the disappearance of pain. With the failure of conservative treatment in young and middle-aged patients, surgery is indicated. The Movshovich operation is reduced to the removal of the affected interspinous ligament and the plasticity of the supraspinous ligament by suturing to the spinous processes in the form of a duplication of the surface sheet of the lumbothoracic fascia, and sometimes the lavsanoplasty of the ligament is performed. On the 2nd month after the operation, a corset is prescribed.
Inflammatory diseases. P.'s inflammatory diseases include Bechterew's disease (see Bechterew's disease), tuberculosis, typhoid, brucellosis spondylitis (see), nonspecific spondylitis, i.e. osteomyelitis of the spine.
Acute osteomyelitis of P. arises usually in the hematogenous way. The causative agent of infection is predominantly Staphylococcus aureus, rarely streptococcus. The lumbar department of P. is most often surprised, and process is localized in arches and shoots, is more rare in bodies of vertebrae. At break of an abscess in the vertebral channel there is a nevrol, a symptomatology. Treatment of P.'s osteomyelitis consists of general and orthopedic. Early massive antibiotic therapy with detoxification therapy usually blocks the inflammatory process. With the ineffectiveness of conservative treatment, surgical treatment is used (see Spondylitis).
Echinococcus P. (bubbly bone cyst) is one of the most frequent bone localizations of echinococcosis (see). The course of the disease is from several months to decades. P.'s defeat can be both primary, and secondary. In the first case, the echinococcal cyst, which developed by hematogenous drift into the vertebral body, further, as a rule, spreads to the soft tissues surrounding P.. In the second case, the echinococcal cyst, located in the mediastinum or retroperitoneal space, subsequently involves P. in the process. P.'s echinococcosis is characterized by a destructive process in the vertebral bodies, most often Thn_v, processes and adjacent parts of the ribs. However, the intervertebral discs suffer little. Usually the patient does not complain. Casoni's reaction is not always positive, so its absence does not indicate an error in the diagnosis. As the echinococcal cyst grows, the bone is destroyed and a breakthrough into the soft tissues may occur. A dangerous complication of a process that proceeds relatively favorably is a breakthrough into the spinal canal. It involves heavy nevrol, disorders. For rentgenol, data (both for primary, and for a secondary multichamber echinococcus) existence of unilateral paravertebral consolidation of spherical outlines is characteristic. The body of the vertebra is first destroyed by the type of small cystic rarefaction, then a massive destructive focus is formed with the destruction of the cortical substance, often with patol, compression. With a breakthrough into soft tissues, the following are characteristic: 1) destruction of the ribs and the transverse process (the head and neck of the rib with the adjacent transverse process); 2) one-sidedness of the lesion; 3) sclerotic border of demarcation; 4) slight damage to the discs; 5) reactive ossification of the longitudinal ligaments.
When an echinococcal focus is detected in the vertebra, surgical treatment is indicated.
With hydatid echinococcus, removal of the cyst leads to the elimination of the process. Operative stabilization of P. (according to indications) allows to restore its support ability. With alveolar echinococcus, the prognosis is much worse, since the radicalness of its removal (even by resection of the vertebral bodies) is always doubtful.
Tumors
There are benign and malignant tumors P. Malignant tumors, in turn, can be primary and secondary (metastatic).
The most frequent benign tumors of P. (in descending order of frequency) include hemangioma (see), osteoblastoclastoma (see), osteochondroma (see.
Rice. Fig. 25. X-ray of the lumbar spine of a patient with hemangioma of the II lumbar vertebra (lateral view): a (before surgery) - the vertebral body is flattened (indicated by an arrow); b (3 years after anterior frontal hemispondylectomy according to Tsivyan) - the body of the II lumbar vertebra is completely replaced by a bone autograft, the bone block is within the I, II and III lumbar vertebrae (limited by arrows).
Hemangioma is more often localized in the bodies of the thoracic vertebrae, less often in the cervical and lumbar. The body of one vertebra is usually affected, rarely two or three. Clinically, hemangioma is manifested by pain, with damage to the arches and processes - radicular and even spinal syndromes. Perhaps the sudden onset of paresis or plegia when the contents of the hemangioma break through the front into the epidural space. At patol, a change there are symptoms of damage to P. The current is more often long. The radiograph shows a cellular or lattice structure with pronounced vertical beams, the contours of the body are even or convex, the sagittal size of the body is increased, the intervertebral spaces are intact. X-ray therapy is generally accepted (see), with spinal complications - laminectomy (see). A radical operation was developed (Ya.L. Tsivyan) - anterior frontal hemispondylectomy or spondylectomy (Fig. 25). The latter is shown in the case of simultaneous defeat of the arcs.
Osteoclastoma occurs in the vertebral bodies, often extending to the area of the arches. Two or more vertebrae may be involved in the process. It is manifested by pain, limited mobility, local soreness, radicular and spinal symptoms are possible. Radiographs show swollen vertebral bodies with a typical cellular structure. X-ray therapy is used for treatment, as well as radical removal of the affected sections or entire vertebrae, followed by their replacement with bone grafts.
Aneurysmal bone cysts are classified as tumor-like formations, they have much in common with osteoblastoclastoma. Differential diagnosis is sometimes very difficult. Treatment is to remove the cyst.
Osteochondroma occurs in all departments of P., comes more often from the articular processes. With growth into the lumen of the spinal canal, it causes its narrowing, while the symptoms of spinal cord compression come to the fore. It is manifested by pain, radicular or spinal syndromes. On P.'s radiographs, a patchy uneven structure of the spongy substance of the vertebral body with a protruding tuberous contour of the vertebra is revealed. Informative, as with other tumors, epidurography (see). Osteochondroma can become malignant. Surgical treatment is radical - more often sagittal hemispondylectomy with bone grafting.
Osteoid-osteoma is clinically characterized by constant increasing paroxysmal pain. On radiographs, a focus of sclerosis in the vertebral body of a stellate shape with a zone of enlightenment is typical. Highly effective surgical treatment (removal of the focus).
Carry to primary malignant tumors reticulosarcoma (see), Ewing's sarcoma (see Ewing's tumor), osteogenic sarcoma (see), chondrosarcoma (see), malignant osteoblastoclastoma, angioendothelioma (see), etc. Klin, and rentgenol. manifestations are highly variable. The pain syndrome and P.'s instability prevail. Pains progress, amplify at night. The prognosis is unfavorable.
Secondary (metastatic) malignant tumors of P. meet very often. Cancer of any localization can give metastases to the P. The most common metastases are cancers of the breast, prostate, kidney, lung cancer. Quite often metastasizes in P. a cancer of such bodies went. - kish. tract, like the pancreas, liver and gallbladder. Metastases of a cancer of a stomach and intestines in P. are rare. Wedge, the picture has no characteristic features. Increasing pain is more common. Sometimes the pain may be absent or disappear. The latter coincides with the destruction of the vertebral body and, apparently, a decrease in intraosseous pressure. X-ray. a picture motley, are frequent patol. fractures of the vertebral bodies.
It is customary to distinguish between osteoclastic and osteosclerotic metastases; there are also metastases of a mixed type. Typical rentgenol, signs of osteoclastic metastases are: 1) destruction of any anatomic element of a vertebra; 2) intactness of the intervertebral discs (lack of narrowing of the X-ray intervertebral fissure); 3) pathological compression with an impression of both (upper and lower) plates; 4) the absence or very small severity of compaction of paravertebral tissues and generally rentgenol, symptoms of germination in soft tissues, as well as from vertebra to vertebra with a characteristic polyfocal lesion. Separate types of tumors may initially give symptoms of expansive growth ("swelling" of the vertebral body). These are the metastases of cancer of the kidney and thyroid gland, with which a slow course is often observed; other metastases progress very rapidly (eg, metastases from pancreatic and lung cancers).
Osteosclerotic metastases are most common in prostate and breast cancer. In these hormone-dependent tumors, osteoclastic metastases sometimes turn into sclerotic ones both under the influence of hormone therapy and spontaneously, as well as from the very beginning, the presence of a mixed type of lesion. The main signs of sclerotic metastases are: 1) diffuse, or spotty, sclerosis of the vertebral bodies, sometimes of the arch and processes; 2) absence patol, compressions; 3) intact discs; 4) sometimes an increase in the size of the body of the affected vertebra. Sclerotic metastases are easily detected radiographically, which cannot be said about diffuse osteoclastic lesions, which, in the absence of patol, compressions and destruction of the cortical substance, can have very poor signs. Very effective in these cases is a layer-by-layer study, as well as the use of computed tomography, which reveals destructive metastases where a conventional radiograph gives negative or questionable results.
Differential diagnosis of metastases (in the sense of referring them to one or another primary tumor) is possible only to a limited extent, taking into account the type of metastasis and the wedge, the picture, especially since the detection of metastasis often precedes the detection of the primary tumor. Considering the difficulties of differential diagnosis between cancer metastases and multiple myeloma (see), it is necessary to examine blood plasma proteins, puncture the sternum, and even better, puncture or biopsy the rib at the site of the radiographically identified focus of destruction. Lymphogranulomatosis (see) with P.'s involvement gives a picture similar to cancer metastases. With lymphogranulomatosis, there is also a secondary lesion of P. due to the germination of tumor tissue from the lymph, nodes and fiber (retroperitoneal, posterior mediastinum) and the formation of marginal destructive foci with the destruction of the cortical substance of the vertebral body, transverse process, and head of the rib.
The main method of differential diagnosis of osteoclastic metastases is the study of other parts of the skeleton, in particular the skull, pelvis, and large tubular bones. Essential for distinguishing osteoclastic metastases from platyspondylia is the syndrome of non-abating and non-alternating pains, with which relatively weak, sometimes completely subsiding pains are observed.
Sclerotic and mixed metastases require differentiation with P.'s lesions with deforming osteodystrophy (see), hemangioma, marble disease (see), osteosclerotic anemia (see Osteomyelofibrosis), some other types of systemic osteosclerosis of focal and diffuse type. In most cases it is reached by rentgenol, researches of other departments of a skeleton.
Treatment of metastatic lesions of P. is symptomatic. With single metastases, it is advisable to promptly remove the affected vertebral body and replace it with a plastic or metal prosthesis, and, less desirable, with a bone graft. At involvement in patol, process of a spinal cord and pains of high intensity - a dissection of sensitive roots.
Operations

Operations on P. are characterized by relatively high trauma, significant blood loss, and increased risk of shock. Anesthesia is usually carried out with the help of endotracheal anesthesia with controlled breathing, which provides sufficient muscle relaxation. Accesses to P. are subdivided into back, posterolateral, anterolateral and front. Posterior approaches are usually used to approach the spinous processes and arches of the vertebrae and are carried out by a linear incision along the midline. From the same access after preliminary laminectomy (see) some interventions on back departments of bodies of vertebrae and intervertebral disks can be executed. Posterolateral accesses are performed most often in the thoracic region in the form of a costotransversectomy (see) and in the lumbar region - in the form of a lumbo-vertebrotomy. Anterolateral and anterior approaches provide best review in most operations on the vertebral bodies and intervertebral discs. In the cervical region, Burghardt and Rozanov's accesses are usually used for this purpose (Fig. 26), differing in their attitude to the muscles and neurovascular bundle of the neck. Used in the chest
Rice. Fig. 29. Schematic representation of the resection of the vertebral bodies in tuberculous spondylitis followed by anterior fusion: a - the affected segment, consisting of two vertebral bodies (the resection border is indicated by a dotted line); b - the graft is inserted into the postoperative defect, blocking the affected area of the spine (circled by a solid line).
Decompressive operations are designed to eliminate compression of the spinal cord and its elements. The most typical decompressive operations are laminectomy and its derivative, hemilaminectomy (removal of half of the vertebral arch). The latter, in combination with a radical intervention on the vertebral bodies, is called "anterohemilaminectomy" or "Seddon's rachiotomy." Spinal cord transposition is sometimes used as a decompressive operation. For example, with scoliosis complicated by paresis or paralysis, half of the arches from the concave side can be resected. The spinal cord at the same time is moved to more direct bed, for reduction of its tension and elimination nevrol, disturbances. A variant of the transposition of the spinal cord - excision of the so-called. the wedge of Urban, i.e., the remains of the vertebral bodies destroyed during tuberculous spondylitis, displaced posteriorly.
Corrective operations are aimed at correcting P.'s deformities and are reduced to a violation of its continuity (complete or partial) using, respectively, vertebrectomy (removal of the entire vertebra), vertebrotomy (dissection or excision of part of the vertebra, Fig. 30) or discotomy (dissection of the disc). Subsequently, one-stage or gradual correction of the curvature (reclination) is performed with simultaneous or delayed stabilization of P. Reclination is carried out using staged plaster casts (see Redressing) or special distractors (see Orthopedic Instruments).
Palliative operations are aimed at eliminating any adverse effects of patol, a process without intervention on the main focus, for example, removal of an intervertebral disc (see Discectomy), which has fallen into the lumen of the spinal canal, with osteochondrosis, posterior spondylodesis with conservative treatment of tuberculous spondylitis.
Andrianov V. L. and Volkov M. V. Tumors and tumor-like dysplastic processes in the spine in children, Tashkent, 1977; Bichem W. P. et al. Clinical study of the joints, trans. from English, M., 1970; Bogdanov F. R., Rokityansky V. I. and Finogenov S. N. Physical methods of treatment in traumatology and orthopedics, p. 142, Kyiv, 1970; Buldakova G. E. Physiotherapy and physiotherapy in the complex treatment of spinal injuries, in the book: Travmat, and orthop., ed. L. P. Sokova and others, p. 57, Barnaul, 1972; Dyachenko V. A. Anomalies in the development of the spine in X-ray anatomical illumination, M., 1949; he, X-ray diagnostics of diseases of bones and joints, M., 1958; Zhedenov VN Comparative anatomy of primates (including humans), p. 65, M., 1962; Zatsepin S. T. and Burdygin V. N. Osteoid osteoma of the spine, Ortop, and traumat., No. 12, p. 4, 1979; Ilizarov G. A. and Markhashov A. M. Blood supply to the spine and the impact on its form of changes in trophism and load: clinical and anatomical and experimental study, Chelyabinsk, 1981; Kaplan A. V. Damage to bones and joints, M., 1979; Kaptelin A. F. Restorative treatment for injuries and deformities of the musculoskeletal system, M., 1969; Knysh I. T. and Volokh G. S. Diagnosis and treatment of primary bone tumors of the sacrococcygeal region, Vestn, hir., t. 110, No. 5, p. 50, 1973; Kolarzh Ya., etc. Primary tumors of the spine, Vestn, rentgenol, and radiol., No 3, p. 12, 1980; Korzh A. A., Talyshinsky R. R. and Khvisyuk N. I. Operative accesses to chest and lumbar vertebrae, M., 1968; Kornev P. G. Osteoarticular tuberculosis, M., 1953; Maykova-Stroganova V. V. and Finkelstein M. A. Bones and joints in the X-ray image, t. 2, L., 1952; Marks V. O. Orthopedic diagnostics, Minsk, 1978; Mitbreit I. M. Spondylolisthesis, M., 1978; Movshovich I. A. Scoliosis, M., 1964; Movshovich I.A. and Vilensky V.N. Polymers in traumatology and orthopedics, p. 115, M., 1978; Reinberg S. A. X-ray diagnostics of diseases of bones and joints, book. 1-2, M., 1964; Rokhlin D. G. X-ray diagnostics of diseases of the joints, parts 1-2, L., 1939 - 1940; Selivanov V. P. and Nikitin M. N. Diagnosis and treatment of dislocations of the cervical vertebrae, M., 1971; Starikova MN et al. Our experience in the complex treatment of patients with uncomplicated compression fractures of the spine, in the book: Pathology of the spine, ed. M. Preisas, p. 230, Vilnius, 1971; Tager I. L. and Dyachenko V. A. X-ray diagnostics of diseases of the spine, M., 1971, bibliogr.; Tager I. L. and Mazo I. S. X-ray diagnostics of displacements of the lumbar vertebrae, M., 1979, bibliogr.; Umyarov G. A. and Andrianov V. L. Osteoblastoclastoma of the spine in children, Ortop, and traumat., No. 6, p. 47, 1968; Watson-Jones R. Fractures of bones and joint damage, trans. from English, M., 1972; Khrisanfova E. N. Evolutionary morphology of the human skeleton, p. 5, M., 1978; Tsivyan Ya. L. Spinal surgery, M. , 1966; he, Injuries of a backbone, M., 1971; he, Operative treatment of humps, M., 1973; Tsyvkin M. V. Aneurysmal bone cyst of the spine, Vopr, neurosurgery., No. 6, p. 43, 1974; he, Surgical treatment of hemangiomas of the spine, in the book: Vopr, bone oncol., ed. M. V. Volkova and S. T. Zatsepin, part 1, p. 139, Moscow, 1977; Chepoy V. M. Inflammatory and degenerative diseases of the spine, M., 1978; Yumashev G. S. and Dmitriev A. E. About the diagnosis of injuries of the ligamentous apparatus of the spine, Vestn. hir., t. 106, No. 5, p. 77, 1971; Brocher J. E. W. Die Wirbelsaulenleiden und ihre Differentialdiagnose, Stuttgart, 1962; Griffin J. B. Benign osteoblastoma of thoracic spine, J. Bone Jt Surg., v. 60-A, p. 833, 1978; Jeddi M. Contribution h l'6tude clinique et radiologique des tumeurs malignes primitives du rachis chez l'enfant, Lyon, 1969; Kohler R. Contrast examination of the lumbar interspinous ligaments, Acta radiol. (Stockh.), v. 52, p. 21, 1959; Raycroft J. F., Hockman R. P. a. Southwick W. O. Metastatic tumors involving the cervical vertebral, surgical palliation, J. Bone Jt Surg., v. 60-A, p. 763, 1978; Rissanen P. M. The surgical anatomy and pathology of the supraspinous and interspinous ligaments of the lumbar spine with special reference to ligament ruptures, Copenhagen, 1960; SchmorlG. u. Junghanns H. Die Gesunde und Kranke wirbelsaule in Rontgenbild und Klinik, Stuttgart, 1957; Steindler A. Post-graduate lectures on orthopedic diagnosis and indications, v. 1-4, Springfield, 1950 - 1954.
I. A. Movshovich; V. P. Illarionov (to lay down. physical.), E. R. Mattis (hir.), I. M. Mitbreit (baln. and physiotherapist.), B. A. Nikityuk (an.), I. L. Tager , L. M. Freidin (rents.), Ya. L. Tsivyan (onc.).
January 29, 2011
From the point of view of biomechanics, the spine is like a kinematic chain consisting of individual links. Each vertebra is connected to the adjacent one at three points: at two intervertebral joints at the back and at the bodies (through the intervertebral disc) at the front. The joints between the articular processes are true joints. Lying one above the other, the vertebrae form two columns - the anterior, built at the expense of the vertebral bodies, and the posterior, formed from the arches and intervertebral joints.
In functional terms, the spine can only be considered in interaction with the ligamentous apparatus and muscles of the body. The normal function of this complex system is possible due to the dynamic balance of all structures.
The mobility of the spine, its elasticity and resilience, the ability to withstand heavy loads are largely provided by the intervertebral discs, which are in close anatomical and functional connection with all the formations of the spine that form the spinal column.
The intervertebral disc plays a leading role in biomechanics, being the "soul" of the movement of the spine. Being a complex anatomical formation, the disc performs the following functions: 1) connection of the vertebrae; 2) ensuring the mobility of the spinal column; 3) protection of the vertebral bodies from permanent trauma (depreciation).
Any pathological process that weakens the function of the disc disrupts the biomechanics of the spine. The functionality of the spine is also impaired.
The anatomical complex, consisting of one intervertebral disc, two adjacent vertebrae with the corresponding joints and ligamentous apparatus at this level, is called the spinal motion segment (SMS) - fig. 1.1, 1.2. 
The intervertebral disc consists of two hyaline plates, tightly adjacent to the endplates of the bodies of adjacent vertebrae, the nucleus pulposus (nucleus pulposus) and the annulus fibrosus (annulus fibrosus). The nucleus pulposus, being a remnant of the dorsal chord, contains the interstitial substance chondrin, a small number of cartilage cells and intertwining collagen fibers, forming a kind of capsule and giving it elasticity. In the center of the nucleus there is a cavity, the volume of which is normally 1-1.5 cm3. The fibrous ring of the intervertebral disc consists of dense connective tissue bundles intertwined in various directions. The central bundles of the fibrous ring are located loosely and gradually pass into the capsule of the nucleus, while the peripheral bundles closely adjoin each other and are introduced into the bone marginal edging. The posterior semicircle of the ring is weaker than the anterior, especially in the lumbar and cervical spine. The lateral and anterior parts of the intervertebral disc protrude slightly beyond the bone tissue, because disc somewhat wider than adjacent vertebral bodies. The anterior longitudinal ligament, being a periosteum, is firmly fused with the vertebral bodies and freely flips over the disc. The posterior longitudinal ligament, which is involved in the formation of the anterior wall of the spinal canal, on the contrary, is freely thrown over the surface of the vertebral bodies and is fused with the disc. Massive in the central part, this ligament becomes thinner outward, i.e. towards the intervertebral foramen. In addition to discs and longitudinal ligaments, the vertebrae are connected by two intervertebral joints formed by articular processes that have features in different departments. These processes limit the intervertebral foramen through which the nerve roots exit. 
The connection of the arches and processes of adjacent vertebrae is carried out by a system of ligaments: yellow, interspinous, supraspinous and intertransverse (Fig. 1.3).
The innervation of the outer sections of the annulus fibrosus, posterior longitudinal ligament, periosteum, capsule, joints, vessels and membranes of the spinal cord is carried out by the Luschka sinuvertebral nerve (p. sinuvertebralis), consisting of sympathetic and somatic fibers (Fig. 1.4). The nutrition of the disk in an adult occurs by diffusion through the hyaline plates.
The listed anatomical features, as well as data of comparative anatomy, allow us to consider the intervertebral disc as a semi-joint, while the nucleus pulposus containing synovial fluid is compared with the joint cavity; the endplates of the vertebrae, covered with hyaline cartilage, are likened to the articular ends, and the fibrous ring is considered as a joint capsule and ligamentous apparatus. This analogy is confirmed in degenerative disc disease (osteochondrosis), which occurs as a typical arthrosis of any joint. 
The static function of the disc is related to cushioning. Discs provide flexibility and smoothness of movement of adjacent vertebrae and the entire spine as a whole. The cushioning ability of the disc is due to elastic mechanisms. The source of the elastic force of the disc is the nucleus pulposus, which has a significant tur-mount and hydrophilicity. According to Fick (1904), the core, absorbing water, is able to increase its volume by 2 times. The nucleus pulposus is under constant pressure in the thickness of the fibrous ring surrounding it on the sides, and the cartilaginous plates above and below.
The desire of the pulpous nucleus to spread is transmitted in the form of uniform pressure on the fibrous ring and hyaline plates (Fig. 1.5). The elasticity of the nucleus, which pushes adjacent vertebrae apart, is balanced by the tension of the fibrous ring connecting the vertebrae, the mass of the human body, and the tone of the muscles of the body. The turgor of the core is variable within a significant range: with a decrease in the load, it increases, and vice versa. Significant core pressure can be judged by the fact that after being in a horizontal position for several hours, the expansion of the disc lengthens the spine by more than 2 cm. It has been established that the difference in human height during the day can reach 4 cm. Decrease in height in old age (up to 7 cm) is due to the loss of hydrophilicity (drying) of the discs. The presence of intradiscal pressure, which increases sharply with exercise, has been experimentally proven on volunteers. Thus, it was found that in the sitting position, the pressure inside the disk L4-5 exceeds 100 kg, i.e. 10-15 kg/cm2. 
The cervical spine is less powerful and more mobile than the lumbar, and in general is subjected to less stress. However, the load per 1 cm2 of the disc in the cervical region is not less, but even more than in the lumbar region. As a result, degenerative lesions of the cervical vertebrae are also common. This position is confirmed by clinical observations.
The resistance of a normal disk to compressive forces is significant. It has been experimentally proved that with a load of 100 kg, the height of the disc decreases by only 1.4 mm, and the width increases by 0.75 mm. To rupture a normal disc, an axial compressive force of 500 kg is required; with osteochondrosis, damage to the disc occurs much earlier (at 200 kg).
The intervertebral disc is a typical hydrostatic system. Because liquids are practically incompressible, then any pressure acting on the nucleus is transformed uniformly in all directions. The fibrous ring, by the tension of its fibers, holds the nucleus and absorbs most of the energy. Due to the elastic properties of the disc, shocks and shocks transmitted to the spine, spinal cord and brain during running, walking, jumping, etc. are significantly softened.
In dynamics, the disk plays the role of a spherical joint, around which the vertebrae move. In this case, a lever of the first degree is obtained, where the core, which is distinguished by high turgor, is the fulcrum. It can be compared to a ball bearing. Even a simple straightening of the spine from a flexion position results in 90-127 kg of pressure on the lumbar discs. If a similar movement is accompanied by a lifting of weight, for example, by an athlete lifting a barbell, then, according to the law of leverage, the load on the disk becomes many times greater than the weight of the object being lifted.
It has been established that in a person weighing 70 kg, holding a load of 15 kg with his hands, with the body tilted forward at an angle of 20 *, the load on the disks L3-4 and L4-5 is 200 kg. If we increase the angle of inclination to 70*, then the same load (15 kg) creates a pressure of 300 kg on the disc, the same as a load of 50 kg with a slight (20e) slope. Lifting a load of 50 kg while tilting the body in the 70s is accompanied by pressure on the disk up to 489 kg.
When holding the load in a vertical position and with slight inclinations, the compression force of the disc is the sum of the weight of the upper half of the body, the weight of the load and the balancing force of the back extensor muscles. At maximum trunk flexion, according to electromyography data, the active activity of the extensor is practically turned off, so the opposing force falls entirely on the ligamentous apparatus of the lumbosacral spine.
Thus, the resulting pressure forces are not excessive to cause damage to healthy intervertebral discs. We observe a different picture in patients with osteochondrosis: they have pain syndrome when they try to lift even a small load (10-20 kg), especially when the torso is tilted forward. In this case, the inertia of the weight of the load has not yet been overcome, and the action of the disk compression forces reaches its maximum.
The elastic and practically non-compressible core of the disc moves in the opposite direction during movement: when the spine is flexed - backwards, when extended - forwards, when lateral bends - towards the convexity.
One of the characteristic features of the spinal column is the presence of four sections, the so-called physiological curvature, located in the sagittal plane:
1. Cervical lordosis, formed by all cervical and upper thoracic vertebrae. The maximum convexity falls on the level of C5 and C6.
2. Thoracic kyphosis. The maximum concavity is at the level of Th5-Th7.
3. Lumbar lordosis, formed by the last thoracic and all lumbar vertebrae. The maximum convexity is at the level of the body L4.
4. Sacrococcygeal kyphosis.
Normally, the sacrum is at an angle of 30° with respect to the frontal axis of the body. The vertical position of a person, in particular, is determined by the position of the pelvic axis and the lumbosacral angle. A pronounced tilt of the pelvis causes lumbar lordosis to maintain balance.
The curvature of the spine is a consequence of the specific features of a person and is due to the vertical position of the torso. When the child begins to raise his head, cervical lordosis appears; begins to sit - thoracic kyphosis; begins to walk - lumbar lordosis. The final formation of bends ends at 15-16 years. Due to the curves, the cervical and lumbar discs are higher in the ventral region, and the thoracic ones in the dorsal region.
The curves of the spine are held by the active strength of the muscles, ligaments and the shape of the vertebrae themselves. This is essential for maintaining a stable balance without wasting muscle power. The spine bent in this way, thanks to its elasticity with spring resistance, withstands the load of the weight of the head, upper limbs and torso. The line of gravity crosses the S-shaped line of the spine in several places.
It is generally accepted that the S-shaped profile of the spine is the result of a person's orthostatic position. It is known that a straight pole is stronger in terms of load than a curved pole, however, with a double camber, the design has a greater strength than a single camber design. The S-shape softens shocks and impacts when moving. The most overloaded arc of the S-shaped spring is the lumbar lordosis, which absorbs the loads of the entire torso and counterloads from the lower extremities and pelvis when a person is in an upright position.
In most people, the line of gravity of the head, upper limbs and torso lies 1.3 cm anterior to the horizontal line drawn through both ear openings.
 The lower back musculature, when standing, counteracts gravity, while the abdominal muscles are passive. Consequently, in most people, the line of gravity runs in front of the spine, and the latter is maintained in a straight position due to reflex contraction of the muscles of the back, so the line of gravity does not increase all the curves of the spine, but rather straightens the lumbar lordosis. When standing, the muscular and ligamentous apparatus of the spine are in a certain tension, putting pressure on the vertebral bodies (Fig. 1.6).
The lower back musculature, when standing, counteracts gravity, while the abdominal muscles are passive. Consequently, in most people, the line of gravity runs in front of the spine, and the latter is maintained in a straight position due to reflex contraction of the muscles of the back, so the line of gravity does not increase all the curves of the spine, but rather straightens the lumbar lordosis. When standing, the muscular and ligamentous apparatus of the spine are in a certain tension, putting pressure on the vertebral bodies (Fig. 1.6).
Currently, the presence of physiological scoliosis of the spine is almost not recognized by anyone. Along with this, one cannot ignore the data of F.F. Ogienko (1971) on the uneven distribution of the load on the intervertebral disc, due to the anatomical asymmetry of the human body: in 60% of people, the left leg is longer than the right, in 20% - on the contrary. The difference in leg length usually does not exceed 1 cm, but nevertheless, when standing, a person rarely loads both legs to the same extent. With a predominant load on the right leg, the pelvis and lumbar spine lean slightly to the left, and the thoracic spine - in the opposite direction (compensatory). At the same time, some rotation of the body occurs, because. the shoulder girdle turns towards the free leg, i.e. to the left. Most people who are right-handed bend not only forward, but also partially to the right when lifting a load. These asymmetries form the biomechanical basis of chronic microtraumatization, mainly of the left posterolateral parts of the disc (stretching of the ring and displacement of the nucleus pulposus in the same direction), and are the cause of the predominance of left-sided localization of pain in lumbar osteochondrosis.
The movements of the spine are due to the contraction of certain muscle groups located in front and behind it. The extensors are significantly larger in mass than the flexors, which is explained by the static load on the spinal column in the vertical position of the body. It has been established that muscles that have an oblique direction of fibers, a large surface of origin and a small extent (they also include the extensors of the back) are able to show greater
force at low voltage. The work of these muscles, counteracting the force of gravity, holds the body in an upright position, tells it one or another pose. These muscles are called by Lesgaft "strong", in contrast to the "dexterous" muscles (for example, the forearm).
Ligaments of the spine in the dynamic aspect serve to inhibit movements in the opposite direction. So, extension is prevented by the anterior longitudinal ligament, flexion is prevented by the posterior longitudinal, interspinous and yellow ligaments, and lateral slopes are intertransverse ligaments. Under normal conditions, there is a physiological balance between the antagonist ligaments. Sometimes the ligaments can withstand a very large load. This is evidenced by the results of electromyographic studies of the back muscles during movements. The EMG activity of the muscles was quite high and was determined during movement, except for the positions of extreme flexion and extreme extension. It was at these moments that the entire load in the form of a tensile force fell entirely on the ligamentous apparatus.
Intervertebral joints limit the free flexibility of the spine, giving it a certain direction. Movements in these paired joints and the disc occur synchronously.
With such an extensive function of the spine, there cannot be much mobility between its individual segments; otherwise, the spine could not serve as a reliable support. In addition, too much mobility between the vertebrae would be dangerous for the spinal cord. At the same time, the movements of many segments, summed up, provide significant mobility of the spine as a whole. The degree of mobility in each segment is directly proportional to the square of the height (thickness) of the disk and inversely proportional to the square of its cross-sectional area. This is clear from a simple example. If we take an elastic rod, then its mobility in the sense of flexion-extension will be the greater, the smaller the cross-sectional plane in relation to the length. The smallest height is at the uppermost cervical and upper thoracic discs. The discs located below this level increase in height, reaching a maximum at the L5-S1 level, so the greatest range of motion is observed in the lumbosacral and lower cervical regions. Extension in these sections is accompanied by some physiological narrowing of the intervertebral foramen due to forward displacement of the articular process of the underlying vertebra.
The least mobility noted in the thoracic region also depends on the inhibitory effects of the ribs connecting the chest into a rather rigid cylinder, as well as on the adjoining of the spinous processes connected to each other by a powerful ligamentous apparatus.
The total length of all discs in newborns is 50% of the length of the spinal column. During growth, the vertebral bodies grow faster than the discs. In adults, the total height of the intervertebral discs is 25% of the length of the spine.
Movements of the spine are carried out along three axes: 1) flexion and extension around the transverse axis; 2) lateral tilts around the sagittal axis; and 3) rotation (turns) of the body around the longitudinal axis. Circular movements are also possible, performed sequentially along all axes.
Rotational movements predominate in the cervical and upper thoracic regions. Flexion and extension reach the greatest extent in the lumbar and cervical regions, lateral movements - in the lower thoracic region. When the spine is flexed, only the thoracic region is practically bent, while the cervical and lumbar regions are straightened, while, on the contrary, the cervical and lumbar regions unbend, and the thoracic region straightens.
In addition, circular motion around intermediate axes is possible, as well as lengthening and shortening of the spine by increasing or smoothing the curves of the spine while contracting or relaxing the corresponding muscles (spring movements).
However, it should be noted that the numerical data, based on the materials of different authors, vary widely. So, for example, the flexion of the spine as a whole varies within 33-200°. These fluctuations are undoubtedly associated with many factors - the degree of muscle training, age and profession, compliance of the ligamentous apparatus, etc.
The static-dynamic apparatus of the spine is under the constant control of the muscles of the whole body: the trunk, abdomen, muscles that connect the trunk with lower limbs, and even under the influence of the respiratory muscles, including the diaphragm.